A 59-year-old female with hypertension and gastroesophageal reflux disease (GERD) presents to the emergency department (ED) with 1 month of severe epigastric discomfort. The pain is episodic and sharp in nature with radiation to her back. Pain is worse after eating and is followed by nausea and vomiting. The patient reports a 20-pound weight loss over the last 6 weeks. Denies drug, alcohol and tobacco use.
Patient was admitted to the hospital and underwent a normal gastric emptying study and colonoscopy. An esophagogastroduodenoscopy (EGD) showed multiple shallows ulcers in the gastric fundus and duodenum. Peptic ulcer disease was treated with a course of proton-pump inhibitor (PPI) therapy. Repeat endoscopy later showed resolution of ulcers. Patient is now being seen in the vascular surgery clinic 6 months after initial presentation. She has lost over 80 pounds secondary to food aversion and severe post-prandial pain.
On physical exam, blood pressure is 128/68 mmHg, pulse is 87 bpm, temperature is 97.9°F, SpO2 is 96% on room air. The patient is in no acute distress, heart rate and rhythm are regular, and no murmurs are appreciated. Lungs are clear to auscultation with normal pulmonary effort. Patient has tenderness on deep palpation to epigastric area. No abdominal bruit, guarding or rebound tenderness is appreciated.
Laboratory work including basic chemistry, complete blood count, troponin, lactate, and lipase are within normal limits. Chest x-ray shows no acute cardiopulmonary disease. Electrocardiogram (ECG) demonstrates normal sinus rhythm.
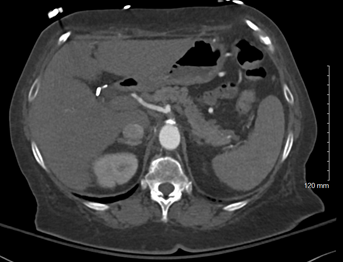
Computed tomography angiography (CTA) demonstrates severe focal stenosis of proximal celiac trunk (Figure 1 and 2) and chronic occlusion of the proximal superior mesenteric artery (SMA) with reconstitution via inferior mesenteric artery (IMA) collaterals. There is no evidence of acute mesenteric ischemia. Imaging is consistent with chronic mesenteric ischemia.
Figure 1
Figure 1
Figure 1. CTA abdomen demonstrating severe focal stenosis of proximal celiac trunk.
Figure 1. CTA abdomen demonstrating severe focal stenosis of proximal celiac trunk.
Figure 2
Figure 2
Figure 2. This patient's focal celiac calcification is consistent with atherosclerotic disease. This is in contrast to celiac narrowing seen in median arcuate ligament compression, which demonstrates a characteristic hooked appearance on CTA.1 This distinction is best appreciated in a sagittal plane.
Figure 2. This patient's focal celiac calcification is consistent with atherosclerotic disease. This is in contrast to celiac narrowing seen in median arcuate ligament compression, which demonstrates a characteristic hooked appearance on CTA.1 This distinction is best appreciated in a sagittal plane.
What is the next step in treatment of this patient's chronic mesenteric ischemia?
Show Answer
The correct answer is: C. Revascularization
Chronic mesenteric ischemia (CMI) is caused by stenosis or occlusion of the mesenteric vasculature causing a mismatch in blood supply and demand within the intestines.2-4 This condition is most commonly caused by the accumulation of atherosclerosis within the proximal portions of the celiac, superior mesenteric or inferior mesenteric artery. Less commonly, this can be caused by dissection, vasculitis, fibromuscular dysplasia, radiation, and cocaine abuse. The same risk factors for atherosclerosis within the coronary arteries or peripheral arteries also contribute to the plaque within mesenteric vessels. These include smoking, hypertension, diabetes mellitus and hypercholesterolemia. Over 70% of patients with CMI are women and the majority are greater than 60 years of age.2
Frequently termed abdominal angina, CMI patients most commonly first present with recurrent post-prandial abdominal pain. This pain often results in substantial weight loss and the development of food aversion. Patients may also experience nausea, vomiting, diarrhea and lower gastrointestinal bleeding secondary to ischemic colitis or gastritis. Typically, pain begins 15-30 minutes after a meal and lasts for up to 30 minutes.2 Classic symptoms occur more frequently when two or more mesenteric vessels are involved.3
When mesenteric ischemia is suspected, diagnostic imaging include abdominal vascular ultrasound, computed tomography (CT)- and magnetic resonance (MR)- angiography and invasive angiography, with CTA being the preferred definitive modality.4 These provide morphology and flow velocities through the vessels.3 Other conditions that can cause postprandial pain should also be excluded with endoscopy and colonoscopy.4 Diagnosis requires both clinical symptoms and mesenteric artery occlusion on imaging. A high index of suspicion is required of clinicians as an average of 15 months passes between start of symptoms and diagnosis of CMI.5
Revascularization is recommended in patients with CMI to resolve associated symptoms and improve quality of life.4 The decision on how to best intervene involves multiple patient specific factors including comorbidities and extent and location of disease. Endovascular repair is recommended as the initial treatment in patients with CMI and suitable lesions.4 Open repair (OR) is reserved for patients who have complex lesions, have experienced endovascular failures and for otherwise young, healthy patients.4,5 This patient has radiographic findings of mesenteric artery occlusion combined with significant weight loss, food aversion and abdominal pain; therefore, revascularization is recommended (Answer C).
(Answer A) All patients with CMI should undergo a comprehensive nutritional evaluation as many experience significant weight loss and therefore, nutritional deficiencies. However, parenteral nutrition is not recommended as a replacement for revascularization as it carries the risk of further clinical decline, bowel infarction and catheter-related infection.4
(Answer B) Patients who have imaging that demonstrates occlusion in the mesenteric vasculature but do not display clinical symptoms should pursue secondary prevention which may include aspirin and lifestyle modifications such as smoking cessation. Antiplatelet therapy is recommended after revascularization with either aspirin or clopidogrel. Dual antiplatelet therapy is not recommended in these patients given increased bleeding risk.4
(Answer D) Systemic anticoagulation is indicated in the setting of an acute mesenteric arterial or venous thrombus.6 Anticoagulation provides no benefit in chronic mesenteric ischemia.
(Answer E) This patient's severe clinical symptoms in the setting of radiographic mesenteric artery occlusive disease warrants revascularization. Intervention aims to resolve symptoms, aid in weight gain, and improve nutrition and prevent bowel infarction. Supportive treatments are not sufficient for this patient.
References
Horton KM, Talamini MA, Fishman EK. Median arcuate ligament syndrome: evaluation with CT angiography. Radiographics 2005;25:1177-82.
Bakhtiar A, Yousphi AS, Ghani AR, Ali Z, Ullah W. Weight loss: a significant cue to the diagnosis of chronic mesenteric ischemia. Cureus 2019;11:e5335.
Keese M, Schmitz-Rixen T, Schmandra T. Chronic mesenteric ischemia: time to remember open revascularization. World J Gastroenterol 2013;19:1333-37.
Huber TS, Björck M, Chandra A, et al. Chronic mesenteric ischemia: clinical practice guidelines from the Society for Vascular Surgery. J Vasc Surg 2021;73:87S-115S.
Oderich GS. Current concepts in the management of chronic mesenteric ischemia. Curr Treat Options Cardiovasc Med 2010;12:117-30.
Bala M, Kashuk J, Moore EE, et al. Acute mesenteric ischemia: guidelines of the World Society of Emergency Surgery. World J Emerg Surg 2017;12:38.