A 40-year-old woman with no known past medical history presented to her primary care provider with 3 months of intermittent atypical chest pain, exertional dyspnea, and a dry cough.
The patient had no history of fever, weight loss, or recent contacts with tuberculosis or other infectious diseases. Her physical exam was unremarkable and she was hemodynamically stable. A differential diagnosis of atypical infection was made at that time. The patient was discharged on analgesia for the chest pain and referred to a pulmonologist for further investigation. The patient's electrocardiogram (ECG), complete blood count, and pulmonary function tests were unremarkable. Her chest X-ray showed left-sided and posterior deviation of the heart associated with elongation of the left border (Snoopy sign). The right heart border was obscured due to thoracic spine superimposition.
A computerized tomography (CT) scan was ordered to further characterize these findings. The CT scan showed complete absence of pericardium on the left side. A small pericardial layer on the right anterolateral portion of the heart over the right atrioventricular (AV) groove was visible. There was displacement of the heart to the left side (levoposition and levorotation). A tongue/pine-like extension of lung parenchyma was seen between the pulmonary artery and aorta. There was interposition of the lung tissue between the left heart base and the diaphragm as a band-like lucent band. A diagnosis of congenital absence of the left pericardium was made and the patient required no further management.
Five years after the CT scan, cardiac magnetic resonance imaging (CMRI) was performed, showing stable absence of the left pericardium. No significant changes from the CT scan were observed in the CMRI.
We present a case of congenital absence of the left pericardium, a rare cardiac manifestation. Imaging modalities played a pivotal role in its diagnosis and exclusion of other diseases and complications.
Figure 1A
Figure 1A
Figure 1A: CT topogram shows leftward and posterior displacement of the cardiac silhouette, straightening and elongated left heart border (Snoopy sign), obscures right heart border by the spine (single arrow). There are radiolucent bands due to interposition of lung tissue between the aortic knob and main pulmonary artery and between the left hemidiaphragm and the base of the heart (double arrows).
Figure 1A: CT topogram shows leftward and posterior displacement of the cardiac silhouette, straightening and elongated left heart border (Snoopy sign), obscures right heart border by the spine (single arrow). There are radiolucent bands due to interposition of lung tissue between the aortic knob and main pulmonary artery and between the left hemidiaphragm and the base of the heart (double arrows).
Figure 1B
Figure 1B
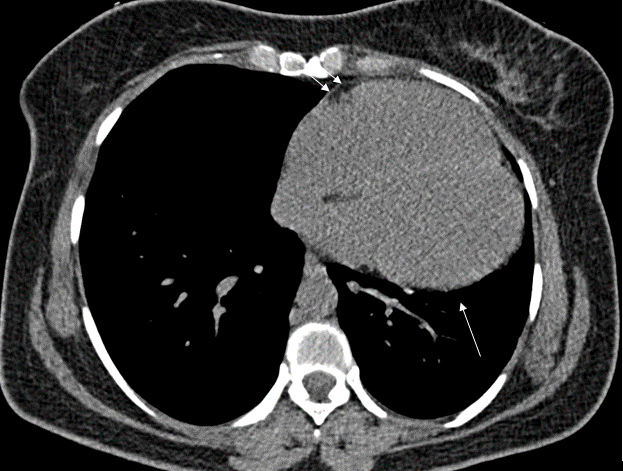
Figure 1B: Axial non-contrast CT scan in the mediastinal window reveals absence of pericardium along the left ventricular border (single arrow). There is a mild presence of the pericardial layer at the level of the right atrioventricular groove (double arrows). There is left sided displacement of the heart (levorotation).
Figure 1B: Axial non-contrast CT scan in the mediastinal window reveals absence of pericardium along the left ventricular border (single arrow). There is a mild presence of the pericardial layer at the level of the right atrioventricular groove (double arrows). There is left sided displacement of the heart (levorotation).
Figure 1C
Figure 1C
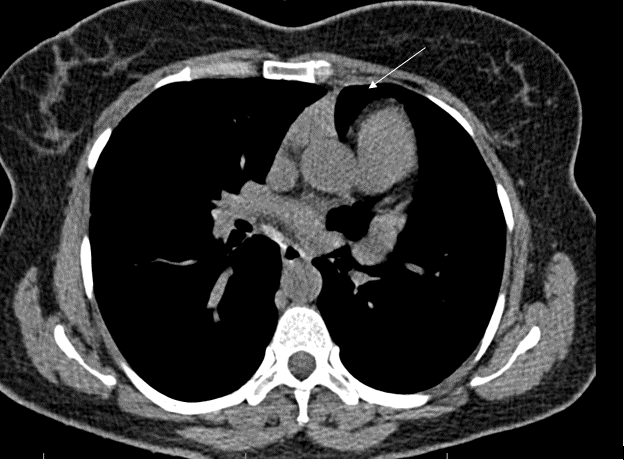
Figure 1C: Axial CT scan in the mediastinal window at level of the main pulmonary artery showing interposition of lung tissue between ascending aorta and main pulmonary artery (arrow).
Figure 1C: Axial CT scan in the mediastinal window at level of the main pulmonary artery showing interposition of lung tissue between ascending aorta and main pulmonary artery (arrow).
Figure 1D
Figure 1D
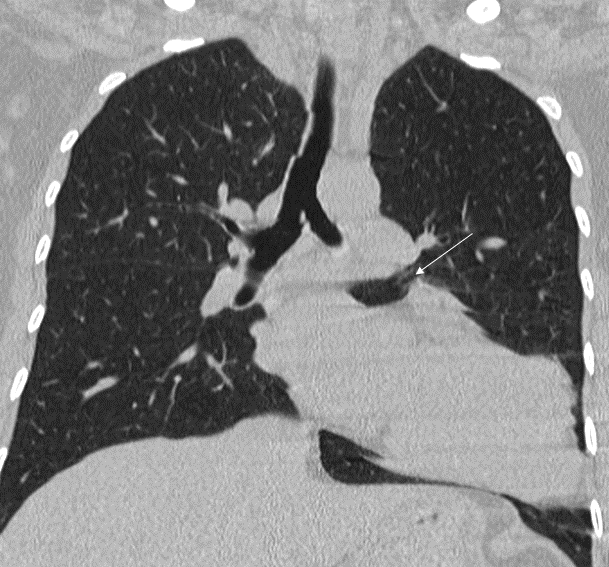
Figure 1D: Coronal CT scan in the parenchymal window showing a tongue-like extension of lung parenchyma between the pulmonary artery and aorta (arrow).
Figure 1D: Coronal CT scan in the parenchymal window showing a tongue-like extension of lung parenchyma between the pulmonary artery and aorta (arrow).
Figure 2A
Figure 2A
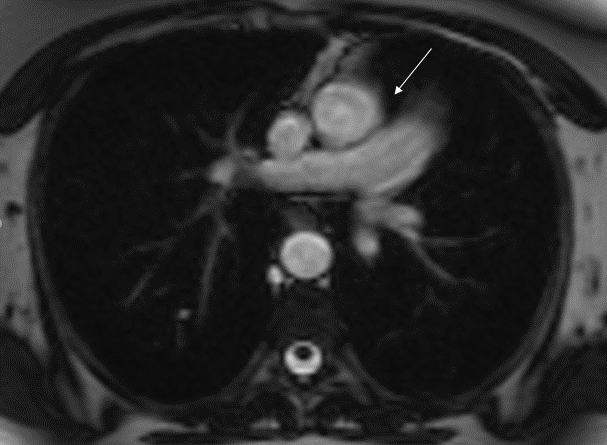
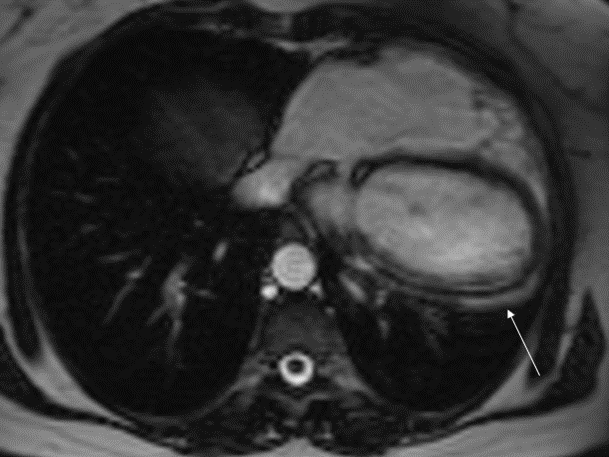
Figure 2A: Follow up CMRI (axial steady state free precession [SSFP] sequence) showing interposition of the lung parenchyma between the ascending aorta and main pulmonary artery.
Figure 2A: Follow up CMRI (axial steady state free precession [SSFP] sequence) showing interposition of the lung parenchyma between the ascending aorta and main pulmonary artery.
Figure 2B
Figure 2B
Figure 2B: Follow up CMRI (axial SSFP sequence) showing levoposition and levorotation of the heart. There is an absence of the pericardial layer along the left ventricle.
Figure 2B: Follow up CMRI (axial SSFP sequence) showing levoposition and levorotation of the heart. There is an absence of the pericardial layer along the left ventricle.
Figure 2C
Figure 2C
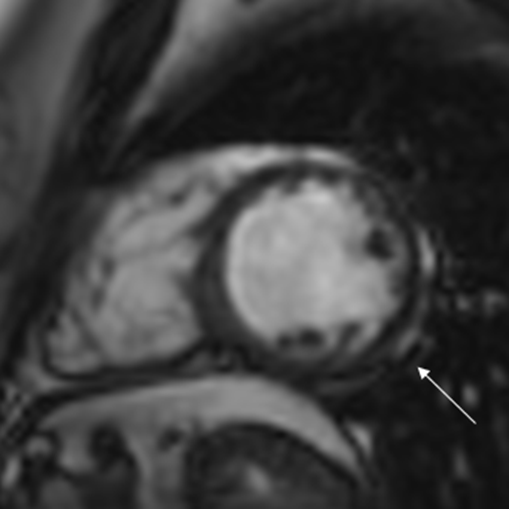
Figure 2C: Follow up CMRI (short-axis SSFP sequence) showing absence of the pericardium over the left ventricle.
Figure 2C: Follow up CMRI (short-axis SSFP sequence) showing absence of the pericardium over the left ventricle.
What is the most likely complication of an isolated absence of the left pericardium?
Show Answer
The correct answer is: A. There are no significant associated risks
Two large autopsy studies indicate an exceedingly rare prevalence of congenital absence of the pericardium with a reported incidence of <1 in 10,000.1 However, because most patients are asymptomatic, and diagnosis is generally incidental, the true prevalence may be underestimated.2 There are three times as many cases in males than females and familial occurrence is rare.1 Complete absence of the left side of the pericardium appears to be the most likely occurrence (prevalent in 67% of cases).2 The developmental condition is due to early atrophy of the left common cardiac vein with limited blood supply to the pleuropericardium.2 Cardiac CT (CCT) or CMRI can be used to help diagnose absence of the pericardium.1 CMRI remains the gold standard modality to assess the pericardium, due to its high sensitivity and spatial resolution.3 However, 10% of patients in the literature with decreased pericardial fat were believed to be mistakenly diagnosed with an absence of the pericardium due to the lack of visualization of the pericardium via CMRI.2
To identify the most likely complication of the complete absence of the left-sided pericardium beyond the literature, the functions of the pericardium must be understood. The pericardium stabilizes and maintains the heart's position within the thoracic cavity, protects the heart from mechanical trauma and infection, and reduces friction at the epicardial surface. It is also thought to prevent pathologic over-distension of the heart.1 These functions are expected to be compromised in the absence of the pericardium. Subsequent cardiac repositioning as seen in complete absences can influence cardiac mobility and ventricular distensibility.3
Interestingly, the complete absence of the pericardium is the least likely of congenital defects of the pericardium to cause complications and has an excellent prognosis.1,4 Seeing that the pericardium, like most connective tissues, plays a functional role, there are natural consequences that can arise. Patients who are symptomatic generally present with atypical chest pain secondary to tension from pleuropericardial adhesions, lack of pericardial cushioning, and undue torsion or strain on the great vessels, as without a pericardium, they serve as the only anchor for the heart.1 The absence of the pericardium can lead to a reduction in ventricular restraint which increases preload in small intervals which can result in ventricular dilatation.2 Cardiac hypermobility can lead to severe tricuspid regurgitation as seen in one report.4,5 Studies of cardiac function have shown that patients with the complete absence of the pericardium have similar ejection fractions to controls.1 These patients also have a normal life expectancy, although, some authors suggest that the cardiac displacement and increased mobility impose an increased risk for traumatic type A aortic dissections.1 Treatment is based on the complications, if any, that can arise.2
For patients with the isolated complete bilateral or complete left-sided absence of the pericardium, no treatment is indicated. In cases of severe symptoms, resolution of chest pain after surgical correction that leads to immobilization of the heart isolates the etiology of the pain to cardiac immobility.1 Considering the lack of widespread data on affiliated risks and the conservative management of this condition, there are no known significant risks associated with the complete absence of the left pericardium.
References
Shah AB, Kronzon I. Congenital defects of the pericardium: a review. Eur Heart J Cardiovasc Imaging 2015;16:821–27.
Abbas AE, Appleton CP, Lui PT, Sweeney JP. Congenital absence of the pericardium: case presentation and review of literature. Int J Cardiol 2005;98:21-25.
Cuccuini M, Lisi F, Consoli A, et al. Congenital defects of pericardium: case reports and review of literature. Ital J Anat Embryol 2013;118:136-50.
Beppu S, Naito H, Matsuhisa M, Miyatake K, Nimura Y. The effects of lying position on ventricular volume in congenital absence of the pericardium. Am Heart J 1990;120:1159-66.
Connolly HM, Click RL, Schattenberg TT, Seward JB, Tajik AJ. Congenital absence of the pericardium: echocardiography as a diagnostic tool. J Am Soc Echocardiogr 1995;8:87-92.