ECG of the Month: Supraventricular Tachycardia: In Search of an Underlying Mechanism (JACC: Case Reports)
Editor's Note: This ECG of the Month was adapted from a JACC: Case Reports ECG Challenge. You can access the original article here.
A 63-year-old woman with a past medical history of hypertension presented to the emergency department with three months of recurrent palpitations. A 12-lead electrocardiogram (ECG) was obtained demonstrating a narrow complex tachycardia (Figure 1A).
Figure 1A
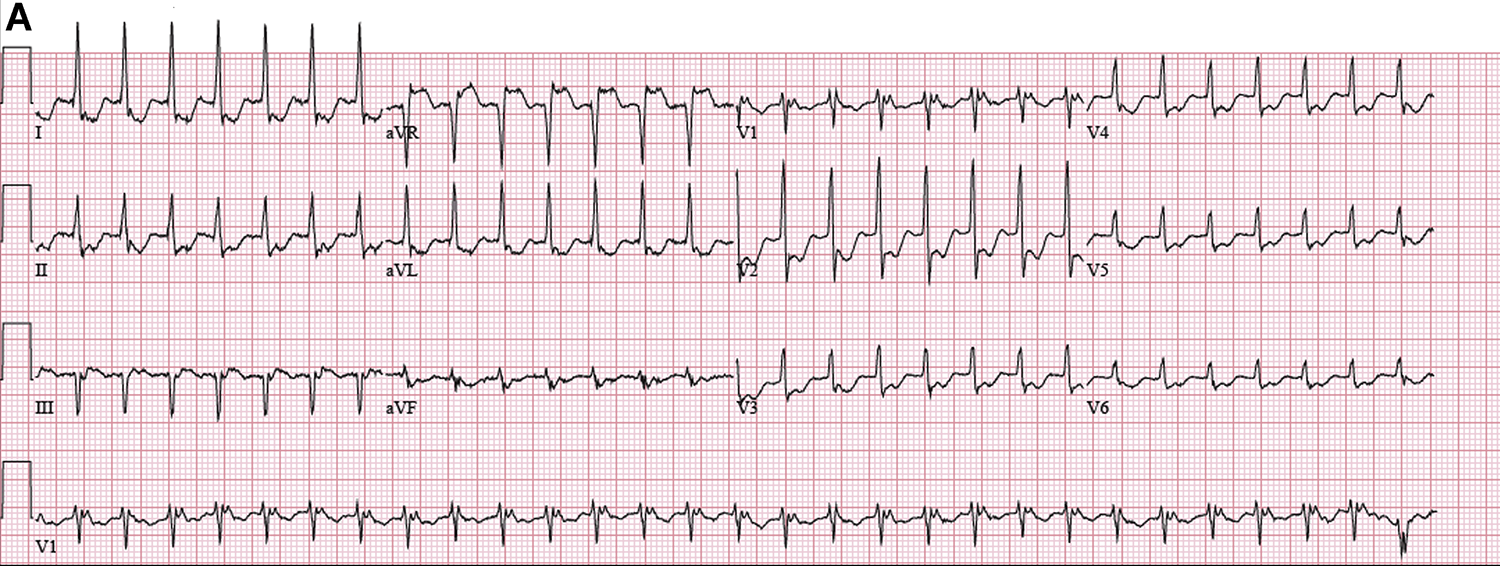
Figure 1A
Figure 1A: 12-Lead Electrocardiogram Demonstrates a Narrow Complex Tachycardia
Figure 1A: 12-Lead Electrocardiogram Demonstrates a Narrow Complex Tachycardia
Which is the diagnosis?
Show Answer
The correct answer is: B. Atrioventricular nodal re-entrant tachycardia (AVNRT).
The differential diagnosis for a regular narrow complex tachycardia is broad,1 and it may not be feasible to definitively exclude any of the above choices. However, often subtle findings on the ECG can help guide one to the correct diagnosis. This is a short R-P tachycardia as shown by P waves at the tail end of the QRS complexes. This is most apparent in lead V1, where the P-wave can mimic an R′ component of the QRS complex, occasionally referred to as a pseudo-R′. Interestingly, detailed inspection of the ECG reveals that the P-waves are intermittently absent (Figure 1B).
The absence of P waves without interruption or perturbation of the tachycardia concludes that the atrium is not a critical component of the tachycardia circuitry. This simple observation excludes sinus tachycardia, AVRT, and AT (wrong answers are A, C, and D) from the differential diagnosis.
The mechanism for typical AVNRT involves dual-AV nodal physiology with antegrade conduction down the slow pathway and retrograde conduction up the fast pathway. Atrial activation is passive, and block to the atrium will not affect the tachycardia and leaves the arrhythmia unperturbed (Figures 1C and 1D).
In contrast, with AVRT, the atrium is a component of the macro-re-entrant circuit, and the absence of atrial activation would result in tachycardia termination (Figure 1E). Sinus tachycardia or AT, in the absence of a P-wave would not be accompanied by a subsequent QRS.
Alternatively, this ECG could be consistent with a junctional tachycardia or a concealed nodofascicular re-entrant tachycardia. These were not answer choices, and although important, are much less common entities. The patient underwent an electrophysiology study which confirmed the presence of dual-AV nodal physiology. The arrhythmia was induced, and diagnostic maneuvers were consistent with a diagnosis of AVNRT. A slow pathway modification was successfully performed, and the patient was non-inducible at conclusion of the case. Detailed inspection of the 12-lead ECG can offer subtle clues to the underlying mechanism of supraventricular tachycardia.
Figure 1B-E
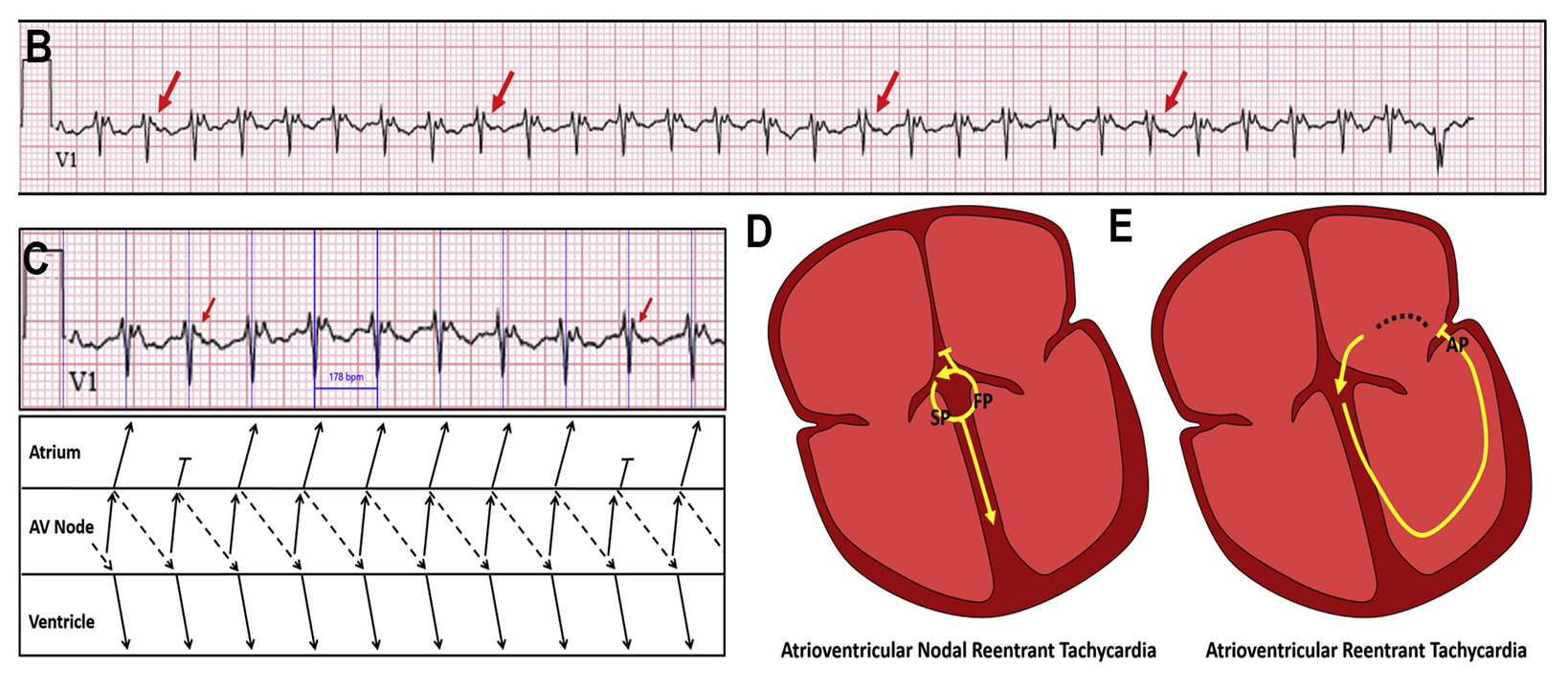
Figure 2
Figure 1: 12-Lead Electrocardiogram Demonstrates a Narrow Complex Tachycardia
Figure 1: 12-Lead Electrocardiogram Demonstrates a Narrow Complex Tachycardia
References
- Katritsis DG, Josephson ME. Differential diagnosis of regular, narrow-QRS tachycardias. Heart Rhythm. 2015;12:1667-76.
Author Information
Jeffrey Smietana, MDElectrophysiology Section, Division of Cardiovascular Medicine
The Hospital of the University of Pennsylvania
Philadelphia, PA
Disclosures
This author has nothing to disclose.