A 65-year-old female patient with a history of diabetes, hypertension, and a family history of bicuspid aortic valve presents with symptomatic severe aortic stenosis (AS) with New York Heart Association Class III symptoms of dyspnea on exertion and a recent heart failure hospitalization. Echocardiography shows left ventricular ejection fraction of 60%, aortic valve area of 0.7 cm2, and mean gradient of 52 mmHg and likely bicuspid valve. Computed tomography confirms a type zero bicuspid valve with moderate leaflet calcification, no significant left ventricular outflow tract or sinotubular junction calcification. There are adequate iliofemoral conduits for transcatheter aortic valve replacement (TAVR), and there is no ascending aortic aneurysm or dilatation. Coronary angiogram shows non-obstructive coronary artery disease. After heart team discussion, the patient is deemed low surgical risk for surgical aortic valve replacement (SAVR). The patient is very concerned about bleeding risk and prefers to avoid long-term anticoagulation.
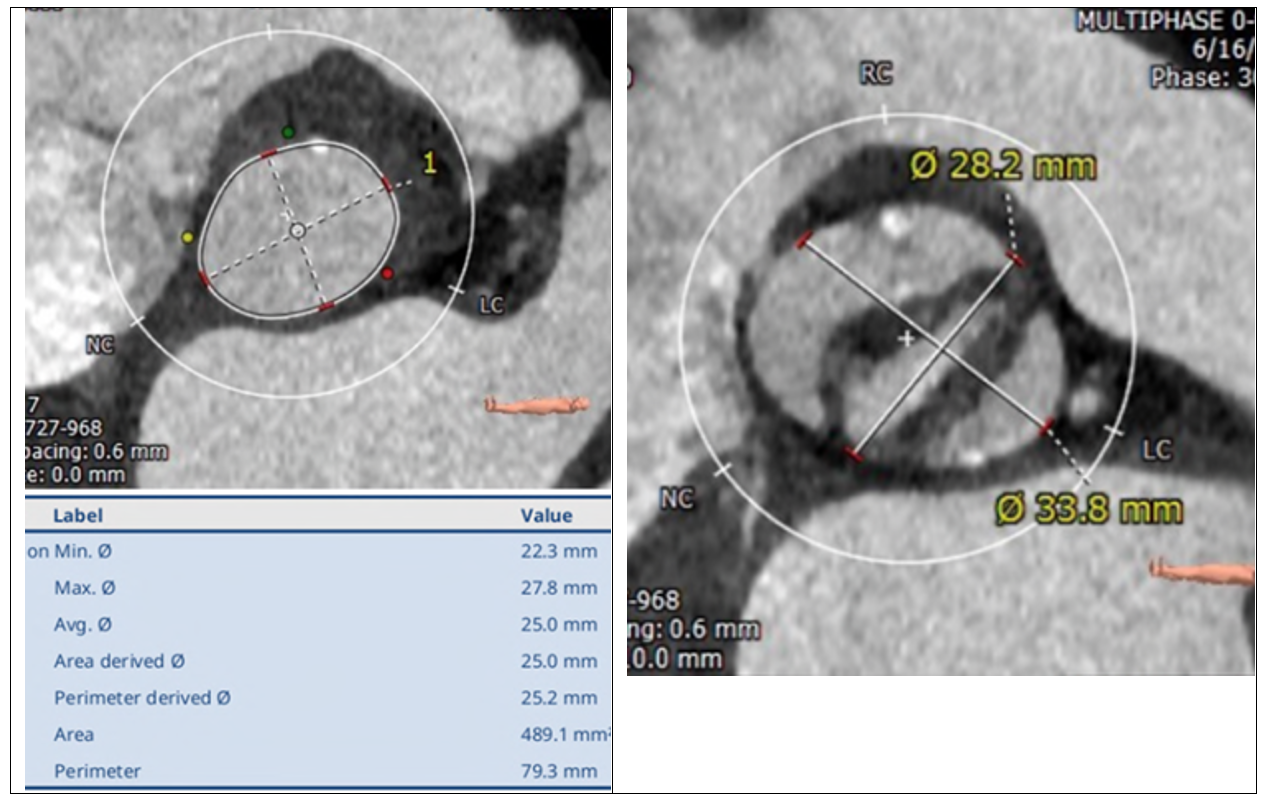
Figure 1
(L): Cardiac Computed Tomography annular reconstruction and (R): view of leaflets/sinuses of Valsalva demonstrating a Sievers Type 0 bicuspid valve.
(L): Cardiac Computed Tomography annular reconstruction and (R): view of leaflets/sinuses of Valsalva demonstrating a Sievers Type 0 bicuspid valve.
What treatment approach would you recommend for this patient?
Show Answer
The correct answer is: B. SAVR with bioprosthetic aortic valve
Given that the patient is low surgical risk, 65 years old, and has symptomatic severe aortic stenosis with type zero bicuspid anatomy, aortic valve replacement is appropriate, and SAVR is preferred over TAVR. Given the patient's age, strong preference to avoid long term anticoagulation and the availability of valve-in-valve TAVR should it be required in subsequent years, a bioprosthetic valve is a reasonable in this case.
American College of Cardiology (ACC)/American Heart Association (AHA) recommendations attribute a class I recommendation to both SAVR and TAVR for patients with severe AS with age 65-80 who are not of high or prohibitive surgical risk.1 The most recent European Society of Cardiology (ESC) guidelines recommend SAVR for patients <75 years who are low surgical risk.2 Although TAVR is widely accepted as an alternative to SAVR in low-risk patients, bicuspid aortic valve patients were excluded from the major clinical trials and therefore represent a separate population. Indeed, ESC guidelines consider a bicuspid aortic valve to be a relative contraindication to TAVR.3 In particular, the shape of the valve and annular complex, as well as the burden of eccentric calcium, create complexities with TAVR valve sizing and sealing which are unique to the bicuspid population. The increased calcium burden may also predispose to higher procedural stroke rates.
Current registry data from Society of Thoracic Surgeons (STS)/ACC Transcatheter Valve Therapies Registry™, which includes all consecutive TAVR procedures performed in the United States (US), suggests that the rates of all-cause mortality are similar at 30 days and 1 year between bicuspid and tricuspid valve groups.4,5 There may be a higher rate of paravalvular leak in bicuspid comparted with tricuspid patients6,7 and a higher rate of pacemaker requirement.5 In low risk patients, stroke rates appear similar between bicuspid and tricuspid aortic valve patients,4,8 however there may be a higher risk of stroke at 30 days when a broader AS population is included.5,9 Ultimately, while bicuspid TAVR outcomes are promising, more robust and randomized data are needed to compare outcomes of TAVR versus SAVR in a bicuspid population to better quantify the relative risks.
Nonetheless, there is increasing national experience for TAVR in bicuspid AS, and TAVR is currently a class 2b indication for severe bicuspid AS in the 2020 ACC/AHA guidelines.1 Indeed, while the data for SAVR remain more robust, TAVR may be considered as an alternative to SAVR after careful consideration by the heart team of patient-specific procedural risks and benefits and patient-specific values and preferences. The importance of heart team involvement and utilizing combined expertise to determine optimal treatment on a case-by-case basis cannot be overrated. As is increasingly the case with many aspects of medical care, the approach to care must be individualized to the patient.
References
Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: Executive Summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2021;77:450-500.
Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2021;Aug 28:[Epub ahead of print].
Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J 2012;33:2451-96.
Forrest JK, Ramlawi B, Deeb GM, et al. Transcatheter aortic valve replacement in low-risk patients with bicuspid aortic valve stenosis. JAMA Cardiol 2021;6:50-57.
Makkar RR, Yoon SH, Leon MB, et al. Association between transcatheter aortic valve replacement for bicuspid vs tricuspid aortic stenosis and mortality or stroke. JAMA 2019;321:2193-202.
Halim SA, Edwards FH, Dai D, et al. Outcomes of transcatheter aortic valve replacement in patients with bicuspid aortic valve disease: a report from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry. Circulation 2020;141:1071-79.
Forrest JK, Kaple RK, Ramlawi B, et al. Transcatheter aortic valve replacement in bicuspid versus tricuspid aortic valves from the STS/ACC TVT Registry. JACC Cardiovasc Interv 2020;13:1749-59.
Waksman R, Craig PE, Torguson R, et al. Transcatheter aortic valve replacement in low-risk patients with symptomatic severe bicuspid aortic valve stenosis. JACC Cardiovasc Interv 2020;13:1019-27.
Medranda GA, Rogers T, Doros G, et al. Transcatheter aortic valve replacement in low-risk bicuspid and tricuspid patients: meta-analysis. Cardiovasc Revasc Med 2021;Jun 25:[Epub ahead of print].