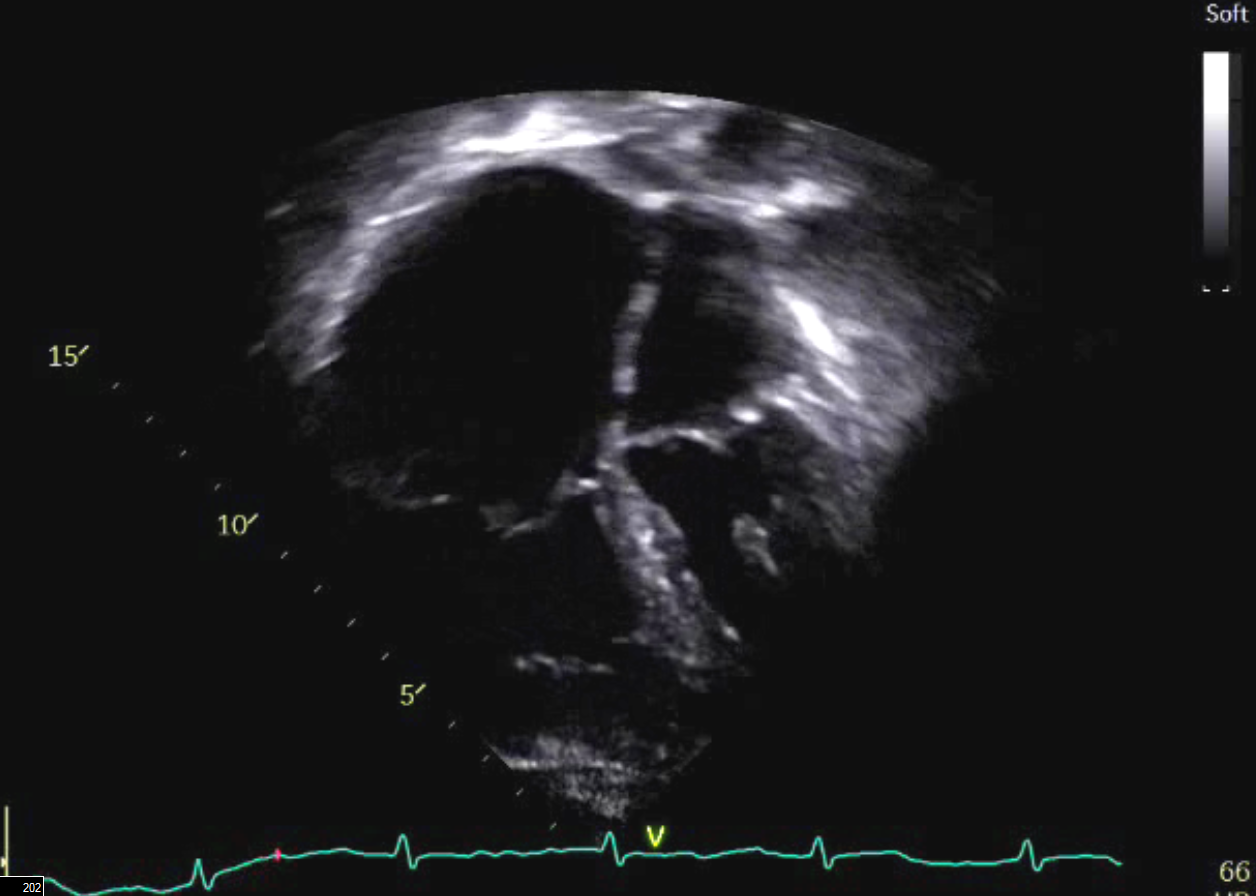
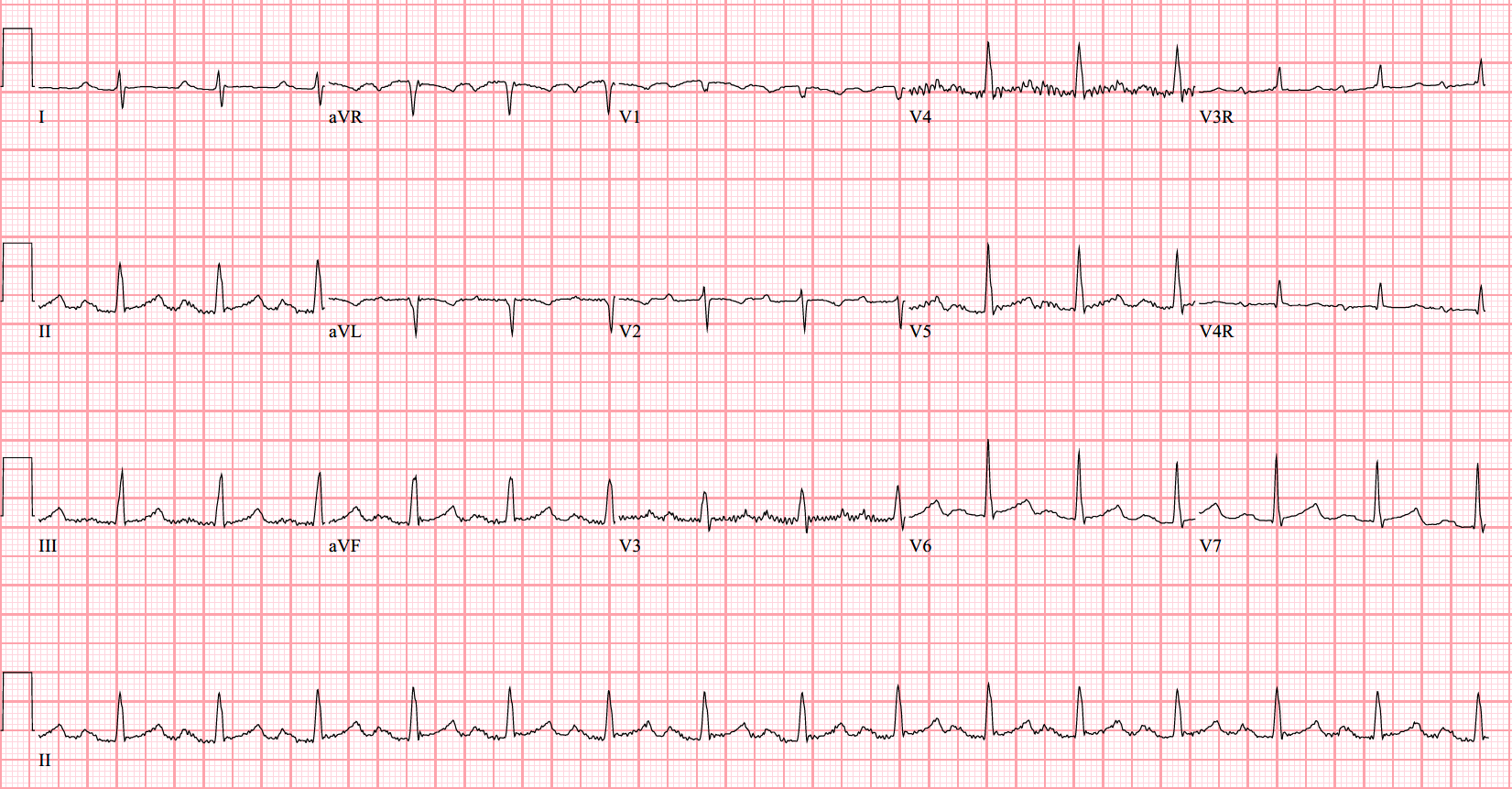
A 63-year-old woman with a history of atrial arrhythmia requiring ablation 10 years ago presented with diverticulitis. During her surgical evaluation, physical exam was significant for a fixed split-second heart sound and a grade III/VI systolic ejection murmur at the left upper sternal border. Room air oxygen saturations were 99%. An echocardiogram revealed a structurally normal heart, with severe right atrial dilation and moderate right ventricular dilation (Figure 1). No significant atrial level shunting was noted. Given the unusual findings, a magnetic resonance imaging (MRI) was performed (Figures 2A-C). At the time of initial diagnosis, she was asymptomatic and active, able to walk or bike approximately 2 miles/three times a week, and surgical intervention was declined. Over the course of a few years, she developed increased fatigability with progressive exercise intolerance, and returned for management. She denied palpitations, chest pain nor syncope. Her electrocardiogram (ECG) is shown (Figure 3).
Figure 1: Echocardiogram
Figure 1: Echocardiogram
Figure 2A: Video of axial stack through the chest
Figure 2A: Video of axial stack through the chest
Figure 2B: Video of coronal stack through the chest
Figure 2B: Video of coronal stack through the chest
Figure 2C: 3D reconstruction
Figure 2C: 3D reconstruction
Figure 3: ECG
Figure 3: ECG
What is the most likely cause for her right heart dilation?
Show Answer
The correct answer is: D. Partial anomalous pulmonary venous return
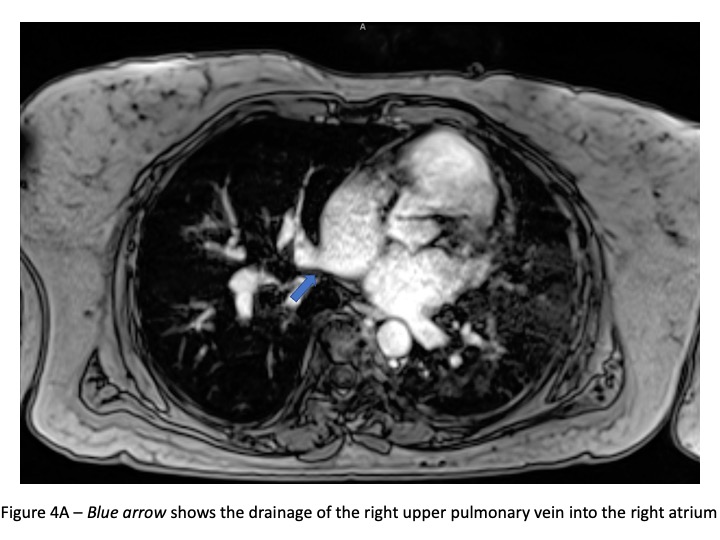
The differential diagnosis of a dilated right heart is broad. The possibilities include Ebstein anomaly, primary pulmonary hypertension, chronic lung disease, arrhythmogenic right ventricular cardiomyopathy, and other congenital heart lesions such as an atrial septal defect or a coronary artery fistula. Though congenital heart disease is less likely in an elderly patient, this should still be considered. The ECG (Figure 3) is non-specific but shows increased right sided voltages and 1st degree heart block. A transthoracic echo showed right heart dilation (Figure 1), but pulmonary vein abnormalities are challenging to ascertain in the setting of sub-optimal echo windows in an elderly patient. A subsequent cardiac MRI confirmed the presence of right heart dilation, and anomalous drainage of the right upper and right lower pulmonary veins into the right atrium (PAPVR) ( Figure 4A-D).
Figure 4A
Figure 4A
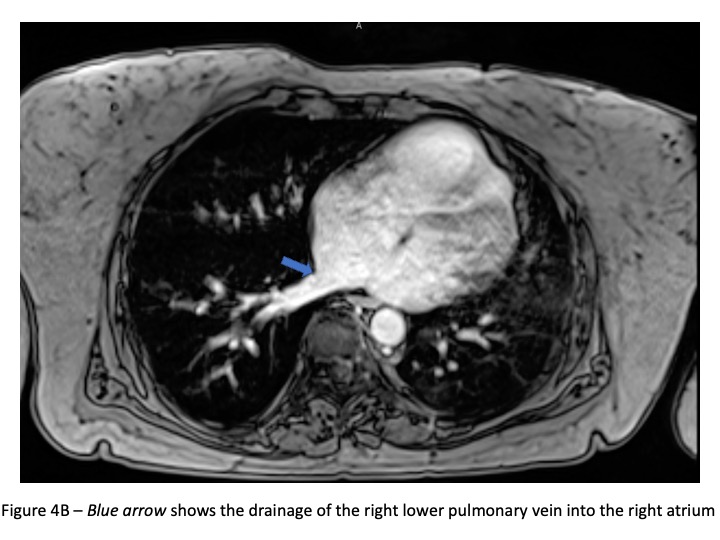
Figure 4B
Figure 4B
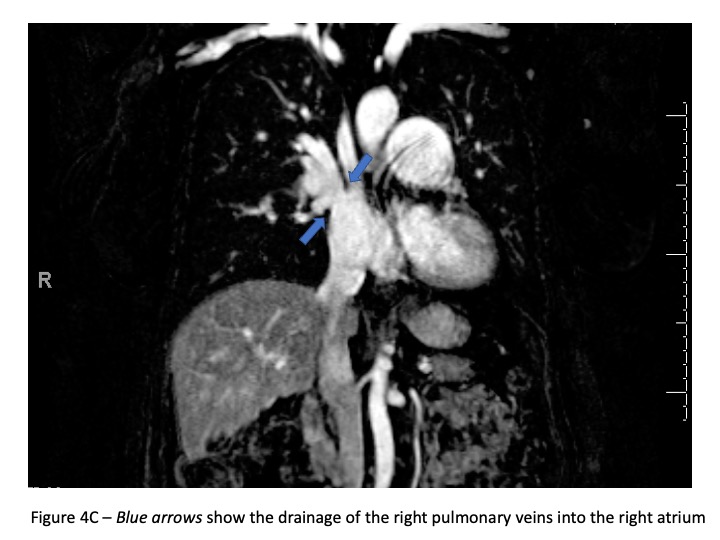
Figure 4C
Figure 4C
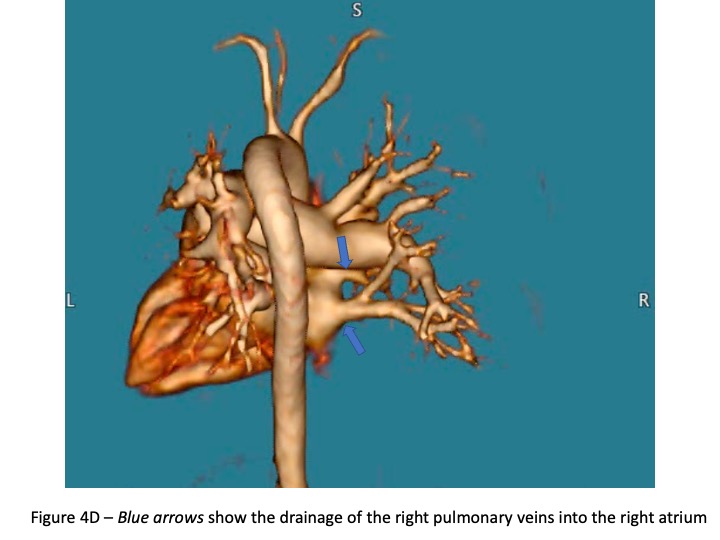
Figure 4D
Figure 4D
PAPVR is a spectrum of disease where one or more, but not all, pulmonary veins are connected and drain anomalously. There is an estimated prevalence of 0.7% of the population by autopsy.1 This number is higher than those clinically detected in life, suggesting that a proportion of patients remain undiagnosed their entire lives. There have been descriptions of all pulmonary veins connecting to various locations other than the left atrium.2 Typically, left sided anomalous veins connect to derivatives of the left cardinal system such as the coronary sinus or the left innominate vein. Right sided anomalous veins tend to connect to derivatives of the right cardinal system, such as the superior (SVC) or inferior vena cava (IVC). The most common PAPVR is of the right sided veins, and particularly that of the right upper lobe inserting into the SVC above or at the drainage of the azygos vein.3
The additional blood volume that the right atrium receives from these anomalous connections is the cause for the right atrial and right ventricle dilation. This is determined by the pulmonary blood flow (Qp) to systemic blood flow (Qs) ratio. The normal ratio is 1:1, as in a normal heart without shunts, the right and left ventricles pump the same amount of blood consistently. The greater the number of anomalous vein connections, the more extra blood flow is obligated to return to the pulmonary circulation before coursing through the systemic circulation. It is most common for right sided PAPVR to be associated with an atrial septal defect (ASD), which contributes to more left to right shunting, in turn making the Qp:Qs even higher. The dilation of the right heart happens progressively and can resolve after surgical repair. If left unrepaired, this volume load and dilation can cause atrial arrhythmias, secondary pulmonary hypertension, and right heart failure. Due to the lower hemodynamic effects of isolated PAPVR without an ASD, these symptoms can be more subtle or not present at all. The indications for repair of PAPVR are most importantly related to symptoms caused by the excess pulmonary blood flow. The hemodynamic effects of an elevated Qp:Qs may result in exercise intolerance, right heart dilation, arrhythmias, pulmonary hypertension, and eventually, right heart failure. A Qp:Qs >2 is considered to be a significant shunt.1,2 In retrospect, the patient's atrial arrhythmias necessitating ablation 10 years ago may have been due to right atrial dilation resulting from PAPVR.
This patient underwent surgical repair a few years after the diagnosis. Intraoperatively, the right upper and middle pulmonary veins were found to connect to the right atrium below the SVC orifice, and the right lower pulmonary vein drained immediately above the IVC. The fossa ovalis was patent and was resected to place a pericardial patch that baffled the right pulmonary veins to the left atrium. She developed atrial tachycardia post operatively and was managed with sotalol. Her right ventricular dilation improved at one-month follow-up. She continues to do well and has resumed all physical activities.
References
Allen HD, Shaddy RE, Pinney DJ, Feltes TF, Cetta F, eds. Moss & Adams' Heart Disease in Infants, Children, and Adolescents, Including the Fetus and Young Adult. 9th ed. Wolters Kluwer Health, 2016.
Pendela VS, Tan BE-X, Chowdhury M, Chow M. Partial anomalous pulmonary venous return presenting in adults: a case series with review of literature. Cureus 2020;12:1-7.
Sormani P, Roghi A, Cereda A, et al. Partial anomalous pulmonary venous return as rare cause of right ventricular dilation: a retrospective analysis. Congenit Heart Dis 2016;11:365-68.