An 18-year old male cross-country runner with recent COVID-19 infection presented for a sports pre-participation evaluation.
Past medical history: attention deficit hyperactivity disorder
Medications: methylphenidate Hcl
History of present illness:
The patient tested positive for COVID-19 after exposure to a known sick contact. He experienced mild symptoms and completed a 10-day quarantine during which he did not exercise. At the end of quarantine, he had two episodes of atypical chest pain with symptoms occurring at rest and lasting 10-15 minutes. The patient was seen in the sports medicine clinic 16 days after his diagnosis and had complete resolution of symptoms.
Vital signs: afebrile, HR 125, BP 108/62
Physical exam: unremarkable besides tachycardia
Electrocardiogram (ECG): sinus tachycardia at 119 bpm, normal intervals, QTc 422ms
Labs: C-reactive protein of 0.6mg/L, sedimentation rate of 2mm/h, troponin I <0.01ng/mL
Transthoracic echocardiogram (TTE) performed approximately 4 weeks from the time of diagnosis: Left ventricular (LV) systolic function was low-normal with ejection fraction (EF) of 51% without regional wall motion abnormality. Global longitudinal strain (GLS) imaging showed reduced peak systolic strain of -12%.
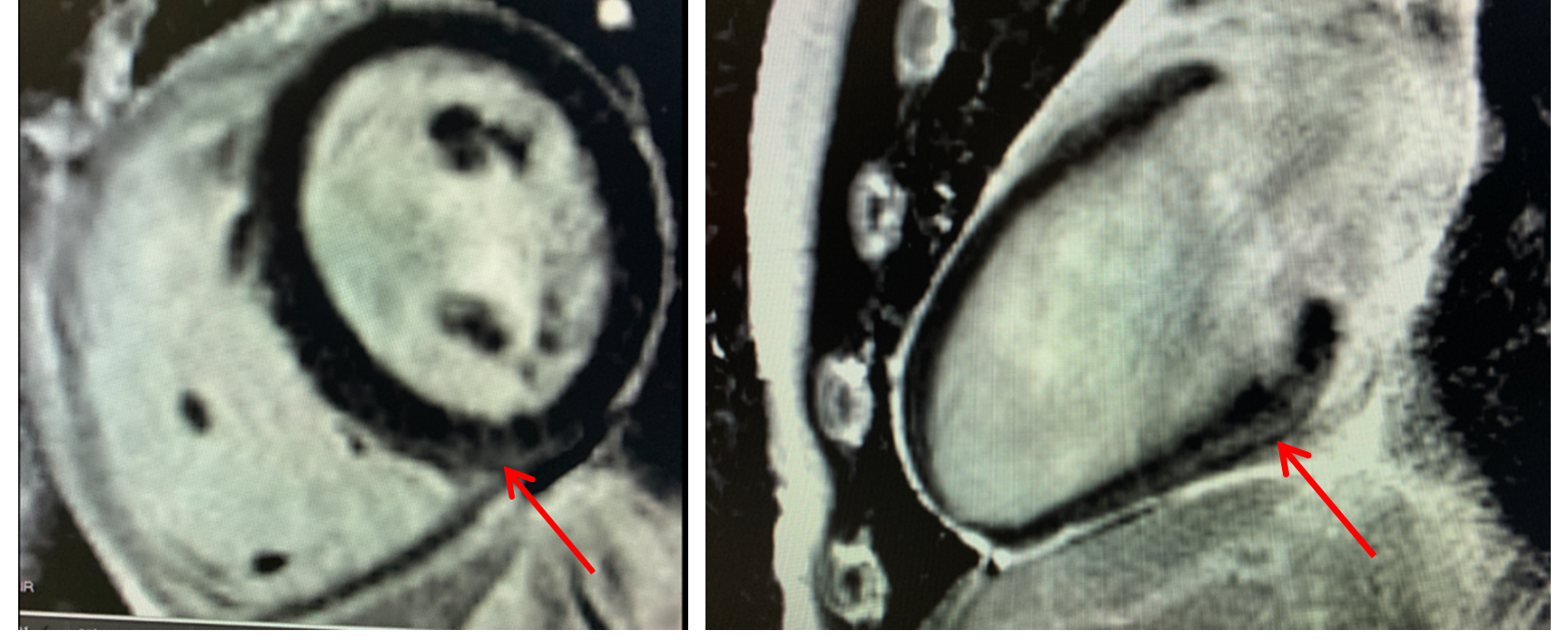
Cardiac magnetic resonance imaging (CMR) performed approximately 7 weeks from the time of diagnosis: Normal LV size and low-normal systolic function (EF 52%), normal right ventricular (RV) size, mildly decreased RV function, and linear sub-epicardial late gadolinium enhancement (LGE) at the basal inferior septum. Mildly elevated native T1 in the basal inferior and inferoseptal segments. Normal global and segmental T2 mapping, indicating absence of edema.
Figures 1 & 2
Figures 1 & 2
When should patient return to play?
Show Answer
The correct answer is: B. 3-6 months
This patient has clinical evidence of myocarditis secondary to COVID-19 infection based on symptoms, tachycardia, and magnetic resonance imaging (MRI) findings. The main concern for this college athlete is risk of sudden cardiac arrest or sudden cardiac death (SCD) with return to play (RTP). Myocarditis is a potential cause of SCD in young competitive athletes accounting for approximately 7% of SCD in this group.1 Currently, a history of COVID-19 is a risk factor for the development of myocarditis even in young, otherwise healthy individuals. Myocardial injury can occur in 7-17% of patients hospitalized with COVID-19 and 22-31% of those admitted to intensive care units.2 However, the overall prevalence of probable or definite cardiac involvement from COVID-19 infection in athletes seems to be much lower. It was estimated to be 0.4-1.5% in a recent report from a multicenter registry of college athletes — the Outcomes Registry for Cardiac Conditions in Athletes (ORCCA).3 Additionally, in a study of 789 professional athletes with prior COVID-19 infection, only 0.5% had confirmed myocardial inflammation.4
The Lake Louise criteria (LLC) encompass a set of CMR findings consistent with acute myocardial inflammation, in patients for whom there is clinical suspicion of myocarditis.5 These criteria were designed to detect myocarditis in patients with symptoms consistent with myocarditis and therefore higher pre-test probability for myocarditis. To date, the largest CMR study of college athletes with prior COVID-19 diagnoses is the Big Ten COVID-19 Cardiac Registry (N=1,597 athletes).6 It is noteworthy that regardless of symptomatology, all athletes underwent CMR, and the LLC were still utilized in this study. Overall 37 athletes (2.3%) were diagnosed with clinical (cardiac symptoms prior to or at the time of testing, N=9, 0.6%) or subclinical (no cardiac symptoms, N=28, 1.7%) myocarditis. It should acknowledge the unknown clinical significance of positive LLC criteria in patients without symptoms and low baseline pre-test probability of myocarditis.
Interestingly, our patient did not meet the LLC for acute myocarditis. However, his CMR was performed 7-weeks after his initial COVID-19 diagnosis. Any myocardial edema our patient may have had likely resolved and was replaced by fibrosis which can be seen in the LGE pattern. In the Big Ten Registry, 27 of the 37 athletes underwent repeat CMR imaging between 4-14 weeks from initial diagnosis. Of the 27, 11 had complete resolution of T2 mapping abnormalities and LGE, and the other 16 had resolution of T2 mapping abnormalities, but persistent LGE. Although our patient lacked classic cardiopulmonary symptoms concerning for acute myocarditis, the persistent sinus tachycardia noted in clinic was an important clue suggesting an underlying pathologic cardiac process necessitating further clinical investigation.
Myocardial fibrosis, and therefore LGE, can also be found in athletes who do not have myocarditis. There are two typical patterns of LGE in healthy athletes: (1) mid-myocardial LGE at the ventricular insertion points or (2) sub-epicardial or mid-myocardial LGE in the inferolateral segments.7,8 It is currently unknown whether these findings are associated with increased risk of adverse events in otherwise healthy, young athletes.
Current guidelines for competitive athletes who have moderate symptoms not requiring hospitalization recommend these patients should abstain from exercise during the symptomatic period.9 They should then undergo evaluation with high sensitivity troponin, 12-lead ECG, and 2D echocardiogram. If any of these are abnormal then there should be consideration for further evaluation with CMR. If the CMR is concerning for myocardial injury, then the RTP guidelines on myocarditis from the American College of Cardiology (ACC)/American Heart Association (AHA) should be followed. These guidelines recommend that athletes with myocarditis should be restricted from exercise for 3-6 months.10 They may RTP once LV systolic function has normalized, serum biomarkers of myocardial injury have normalized, and any clinically relevant arrhythmias on ECG monitoring or exercise stress testing have resolved. Notably, the clinical significance of persistent LGE in asymptomatic athletes with prior myocarditis is unknown, so these athletes should continue to be monitored.
References
Maron BJ, Haas TS, Ahluwalia A, Murphy CJ, Garberich RF. Demographics and epidemiology of sudden deaths in young competitive athletes: from the United States National Registry. Am J Med 2016;129:1170-77.
Huang L, Zhao P, Tang D, et al. Cardiac involvement in patients recovered from COVID-2019 identified using magnetic resonance imaging. JACC Cardiovasc Imaging 2020;13:2330-39.
Moulson N, Petek BJ, Drezner JA, et al. SARS-CoV-2 cardiac involvement in young competitive athletes. Circulation 2021;144:256-66.
Martinez MW, Tucker AM, Bloom OJ, et al. Prevalence of inflammatory heart disease among professional athletes with prior COVID-19 infection who received systematic return-to-play cardiac screening. JAMA Cardiol 2021;6:745–52.
Ferreira VM, Schulz-Menger J, Holmvang G, et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: expert recommendations. J Am Coll Cardiol 2018;72:3158-76.
Daniels CJ, Rajpal S, Greenshields JT, et al. Prevalence of clinical and subclinical myocarditis in competitive athletes with recent SARS-CoV-2 infection: results from the Big Ten COVID-19 Cardiac Registry. JAMA Cardiol 2021;6:1078-87.
Małek ŁA, Bucciarelli-Ducci C. Myocardial fibrosis in athletes ̶ current perspective. Clin Cardiol 2020;43:882-88.
Domenech-Ximenos, B, Sanz-de la Garza M, Prat-González S, et al. Prevalence and pattern of cardiovascular magnetic resonance late gadolinium enhancement in highly trained endurance athletes. J Cardiovasc Magn Reson 2020;22:62.
Kim JH, Levine BD, Phelan D, et al. Coronavirus disease 2019 and the athletic heart: emerging perspectives on pathology, risks, and return to play. JAMA Cardiol 2021;6:219-27.
Pellicia A, Solberg EE, Papadakis M, et al. Recommendations for participation in competitive and leisure sports in athletes with cardiomyopathies, myocarditis, and pericarditis: position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur Heart J 2019;40:19-33.