Editor's Note: This ECG of the Month was adapted from a JACC: Case Reports ECG Challenge. You can access the original articlehere.
A 51-year-old man with severe left ventricular hypertrophy (LVH) was referred to cardiology clinic. Aside from palpitations, he was asymptomatic. He had no known family history of cardiomyopathy, arrhythmia, or sudden cardiac death. Figure 1 demonstrates his baseline electrocardiogram (ECG) (Figure 1A) and ECG in tachycardia (Figure 1B).
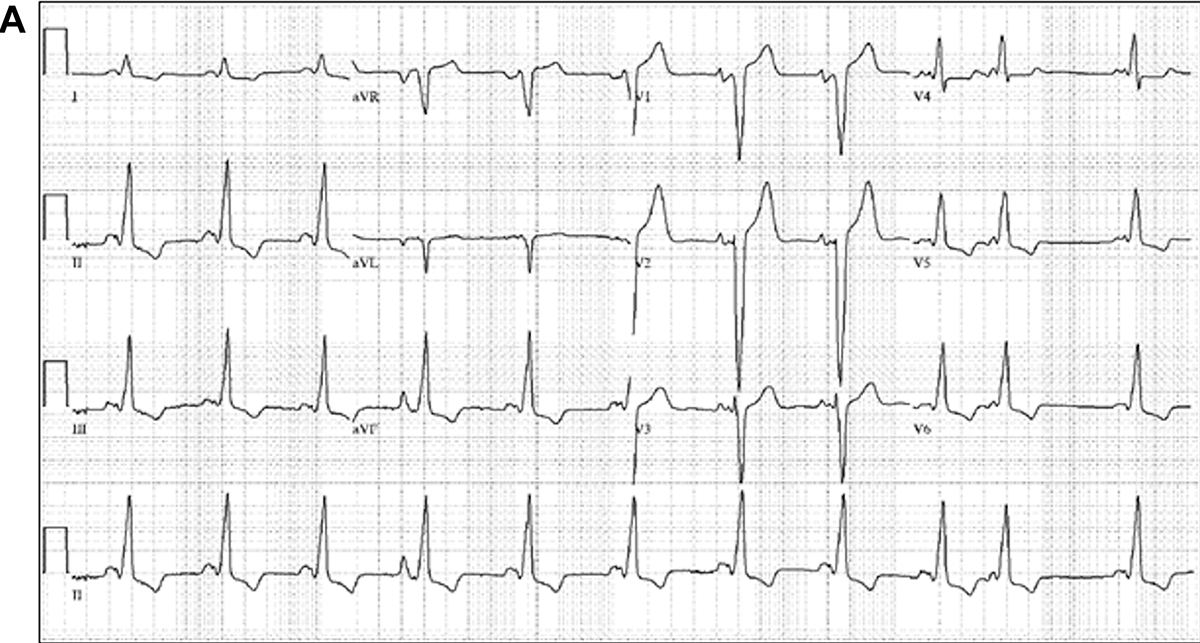
Figure 1A: Baseline electrocardiography
Figure 1A
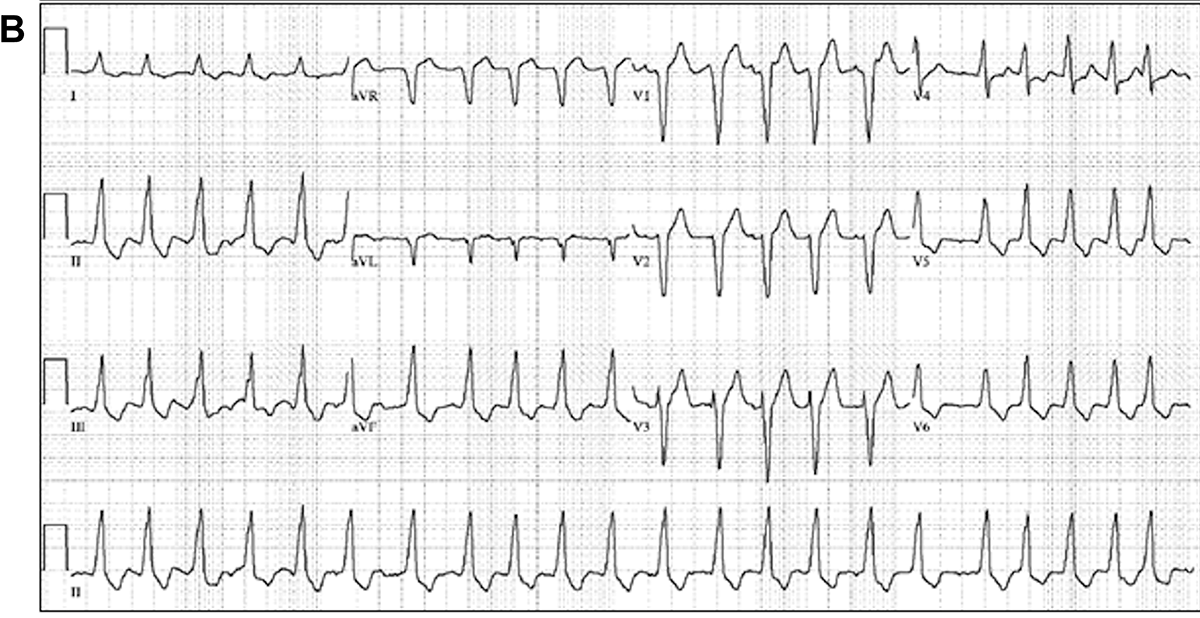
Figure 1B: Electrocardiography in tachycardia
Figure 1B
What is the diagnosis?
Show Answer
The correct answer is: D. HCM with a fasciculo-ventricular AP.
Baseline ECG shows sinus rhythm and a wide QRS complex with left bundle branch block-type morphology. A short PR interval and delta wave are present, confirming ventricular pre-excitation and excluding aberrant conduction (excludes answer A). The QRS precordial transition at V4 and positive delta wave frontal axis localize the accessory pathway (AP) to the anterolateral right ventricle.1 However, two additional electrocardiographic clues are important to note. In Figure 1A, pre-excitation is fixed after a premature atrial complex (PAC). In Figure 1B, the patient is in atrial fibrillation (AF) (excludes answer C). Despite varying RR intervals, pre-excitation is fixed with the same pre-excited QRS morphology as in the sinus ECG.
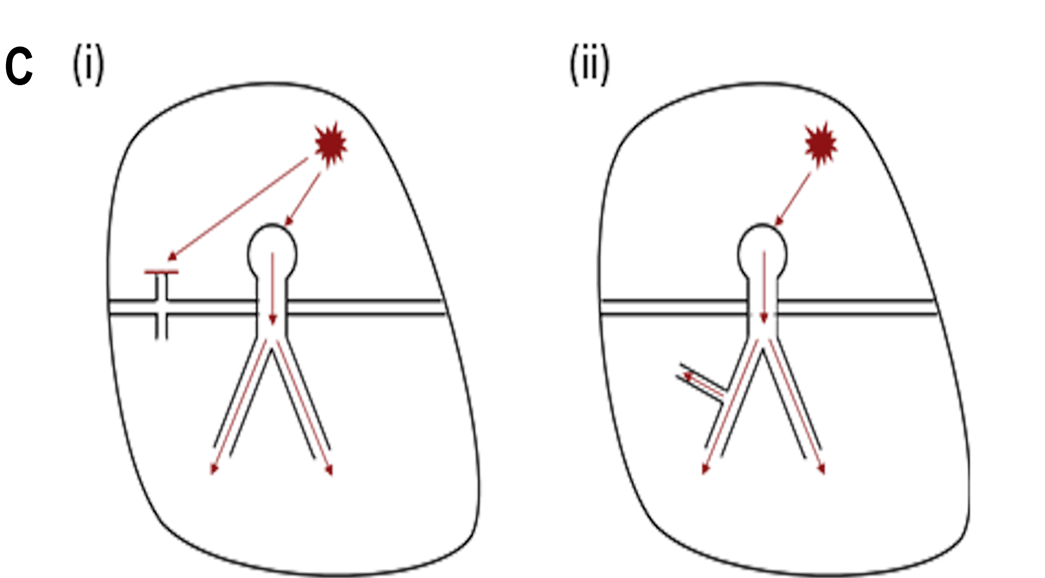
Fixed pre-excitation in the setting of a PAC and AF with varying RR intervals is a diagnostic feature of a fasciculo-ventricular pathway (FVP). FVPs are infranodal connections between a bundle branch and the ventricular myocardium. Figure 1C shows the effect of a PAC on pre-excitation in the setting of a typical atrioventricular AP and an FVP. Typical atrioventricular APs have different refractory periods than those of the AV node (AVN). Thus, a PAC will encounter either a more refractory AVN, resulting in greater pre-excitation, or a more refractory AP, resulting in less or no pre-excitation. On the other hand, an FVP is infranodal. Hence, a PAC will conduct through the AVN unchanged and will not affect the degree of pre-excitation as seen in the current patient. Similarly, AF would have conducted variably down the AV node and typical atrioventricular AP, resulting in beat-to-beat variations in QRS morphology and degree of pre-excitation (excludes answers B and E) but fixed pre-excitation in AF with an FVP (correct answer is D).
The clinical picture of LVH and pre-excitation raises suspicion for familial forms of pre-excitation associated with LVH which include mutation in the PRKAG2 gene, Danon disease, and Fabry disease, among others.2 Initially there was high suspicion for the PRKAG2 mutation because APs are prevalent in this disease and because the referring institution had diagnosed this patient as carrying the PRKAG2 mutation prior to referral. However, repeated genetic testing at the authors' institution identified a pathogenic variant in myosin essential light chain 3 (MYL3), confirming a diagnosis of HCM.
The PRKAG2 mutation disease is rare, resulting from mutations in adenosine monophosphate-activated protein kinase, which regulates glucose and fatty acid metabolism.3 Manifestations include LVH, ventricular pre-excitation, atrial tachyarrhythmias, bradycardia, and conduction disease.3 Danon and Fabry diseases have similar clinical pictures, however, both commonly have extracardiac features not present in the current patient.2
Figure 1C:The effect of a premature atrial contraction on pre-excitation in the setting of a (i) typical atrioventricular bypass tract and (ii) fasciculo-ventricular bypass tract.
Figure 1C
References
Fitzpatrick AP, Gonzalez RP, Lesh MD, Modin GW, Lee RJ, Scheinman MM. New algorithm for the localization of accessory atrioventricular connections using a baseline electrocardiogram. J Am Coll Cardiol 1994;23:107-16.
Koneru JN, Wood MA, Ellenbogen KA. Rare forms of preexcitation: a case study and brief overview of familial forms of preexcitation. Circ Arrhythm Electrophysiol 2012;5:e82-7.
Porto AG, Brun F, Severini GM, et al. Clinical spectrum of PRKAG2 syndrome. Circ Arrhythm Electrophysiol 2016;9:e003121.
Author Information
Stacey J. Howell, MD University of California - San Francisco San Francisco, CA Disclosures This author has nothing to disclose.
Babak Nazer, MD Knight Cardiovascular Institute
Oregon Health and Science University Portland, OR Disclosures This author has nothing to disclose.