Editor's Note: This ECG of the Month was adapted from a JACC: Case Reports ECG Challenge. You can access the original articlehere.
An 18-year-old man with a history of motor vehicle accident complicated by subarachnoid hemorrhage and quadriplegia presented to the hospital with hypoxic respiratory failure and sepsis secondary to aspiration pneumonia. The patient spent 1 month in the intensive care unit and required mechanical ventilation. Following extubation, the patient had recurrent aspiration events as he was unable to clear oral and gastric secretions from his airway. His stay was further complicated by nosocomial coronavirus disease-2019 infection and new aspiration pneumonia. His telemetry monitoring showed changes with tachycardia and T-wave changes. The 12-lead electrocardiogram (ECG) that was obtained is shown in Figure 1.
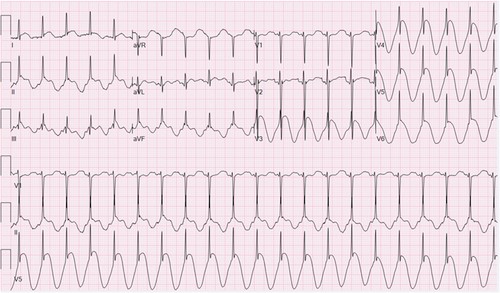
Figure 1: Electrocardiogram Obtained During Hospitalization
Figure 1
The following are shown: pseudo ST-segment elevations, which begin prior to the QRS complex, seen in nearly all leads and most notably in V3-V6. Pseudo ST-segment depressions with similar pattern are noted in aVR and V1. Heart rate is regular at 126 beats/min.
This ECG pattern is mostly associated with which of the following?
Show Answer
The correct answer is: C. Increased intrathoracic or intra-abdominal pressure.
The pattern shown in the ECG in Figure 1 is known as the "spiked helmet" sign. It is recognized by its dome-and-spike or sine-wave-like appearance, with QRS complexes forming spike-like protrusions. It gets its name from its resemblance to the Pickelhaube, the helmet worn by soldiers in late 19th century Prussia.1 The sign shows a pseudo ST-segment elevation, but the elevation is in fact associated with upsloping that begins prior to the QRS complex, which is inconsistent with ischemia. Although often described in the inferior leads, it has been observed in other leads as well. The QRS complex is notably well preserved but appears buried in the dome shape, and the P waves are usually not visible. The presence of the QRS complex helps separate it from other sine-wave-like patterns seen in hyperkalemia or torsade de pointes. The spiked helmet sign is a recently described ECG finding and is often associated with critical illness and a high risk of mortality. It has also been associated with increased intrathoracic or intra-abdominal pressures, sepsis, respiratory distress, subarachnoid hemorrhage, and anoxic brain injury.2 It is not a sign of cardiac pathology and is usually self-limited without any lasting ECG changes.1,2 Although the exact mechanism behind it is not fully understood, diaphragmatic breathing, synchronization of the cardiac pulse with pulsatile diaphragmatic contractions, and repetitive epidermal stretching have all been suggested as potential factors playing a role in the development of the sign.1,2 In this case, the patient was in a critical state, had a history of subarachnoid hemorrhage, and was being treated for severe lung infections, which are all features associated with the spiked helmet sign.
References
Littmann L, Monroe MH. The "spiked helmet" sign: a new electrocardiographic marker of critical illness and high risk of death. Mayo Clin Proc 2011;86:1245-6.
Oluyadi F, Kariyanna PT, Jayarangaiah A, Celenza-Salvatore J, McFarlane IM. Helmet sign on EKG: a rare indicator of poor prognosis in critically ill patients. Am J Med Case Rep 2019;7:260-3.
Author Information
Hani Hamade, MD
Department of Internal Medicine
Metrohealth Campus of Case-Western Reserve University
Cleveland, OH
Disclosures
This author has nothing to disclose.
Ahmad Jabri, MD
Heart and Vascular Center
Metrohealth Campus of Case-Western Reserve University
Cleveland, OH
Disclosures
This author has nothing to disclose.
Adnan Yusaf, MD
Heart and Vascular Center
Metrohealth Campus of Case-Western Reserve University
Cleveland, OH
Disclosures
This author has nothing to disclose.
Mohamed Farhan Nasser, MD
Heart and Vascular Center
Metrohealth Campus of Case-Western Reserve University
Cleveland, OH
Disclosures
This author has nothing to disclose.
Saima Karim, DO
Heart and Vascular Center
Metrohealth Campus of Case-Western Reserve University
Cleveland, OH
Disclosures
This author has nothing to disclose.