An Agitated Heart
With one minute remaining in the first quarter, a 16-year-old male was hit by a lacrosse ball just under his left nipple. He collapsed a few seconds after being hit and was unresponsive when approached by first responders.
He is 73 inches tall, weighs 195 pounds and is a three-sport athlete including playing defense on the varsity lacrosse team as a freshman. He has no prior relevant medical history and has never had any exertional symptoms or limitations. He felt well that day and had no recent illnesses. There is no family history of channelopathies, sudden cardiac arrest/death, unexplained syncope, or cardiomyopathies.
What is the most likely diagnosis?
Show Answer
The correct answer is: B. Commotio Cordis
Given the clinical description of collapse seconds after being hit in the chest, commotio cordis is the most likely diagnosis, making prompt recognition and application of an automated external defibrillator (AED) critical to maximize the chance of survival. This athlete was at a school that had a well-developed emergency action plan (EAP) with an AED onsite. Cardiopulmonary resuscitation (CPR) was initiated within 1 minute of collapse, AED applied, rhythm analyzed (Figure 1), shock delivered, and return of spontaneous circulation (ROSC) was achieved within 3 minutes from the time of collapse.
Figure 1: AED Rhythm Analysis Showing Ventricular Fibrillation
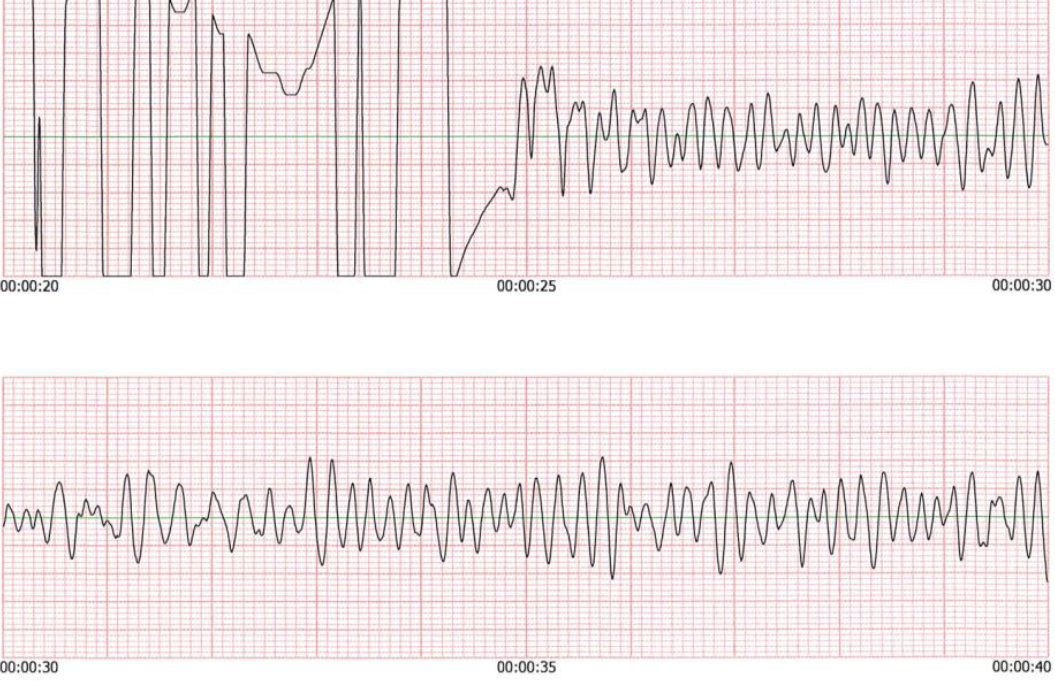
Figure 1
Commotio cordis, or agitation of the heart in Latin, occurs when a sudden, non-penetrating blunt impact to the left chest causes sudden cardiac arrest. Collapse occurs within a few seconds of impact and the presenting rhythm is typically ventricular fibrillation (VF). This first series was published in 1995 reporting 25 cases of commotio cordis.1 The National Commotio Cordis Registry was created in 1996 and since then more than 260 cases of sudden death from chest impact have been reported.2,3 Current estimates of incidence range from 10 to 20 events a year nationally.4 Commotio cordis primarily occurs in thin young males (95% of cases) with a median age of 14 years.5,6 It is most common during participation in sports involving a small projectile with a dense core, such as baseball, cricket, hockey, and lacrosse. A developing, more compliant chest wall is felt to contribute to susceptibility, but the incidence likely also decreases with age given there are less athletes participating in sport with projectiles after high school.
Electrical mechanisms have been studied and instantaneous VF can be induced with low impact blows to the chest during a 20-millisecond window during the upslope of the T wave in an experimental swine model.7 Research has shown that the combination of critical variables, including shape and hardness of the object, the speed of the object, the timing of chest contact and location/orientation of the blow from the object, are all necessary to induce VF with impact.4 Circular shapes with a greater hardness and smaller diameter projectiles at a particular speed (typically ~40mph) with direct impact to left chest wall are most likely to induce VF.8 While commotio cordis is most commonly seen with direct perpendicular blow to the chest wall, impact near the left ventricle (LV) apex/nipple area can, in rare instances, prompt VF.9
The risk of commotio cordis can be attenuated by three means: minimizing chest blows, chest wall protection, and softening the ball. In lacrosse, athletes should be encouraged to avoid hits to the chest but given the nature of the sport, chest blows cannot be completely prevented. While softening the ball decreases the risk, it does not obviate the risk of commotio cordis and may not be feasible in lacrosse. Prior commercially available chest protectors did not lower the risk of commotio cordis10 but newly developed chest protectors can provide increased protection against the development of commotio cordis. These new chest protectors are approved by the National Operating Committee on Standards for Athletic Equipment (NOCSAE). USA Lacrosse, the National Federation of State High School Associations, and the National Collegiate Athletic Association (NCAA) require all goalies in girls' and boys' lacrosse to wear protectors that meet the new NOCSAE standard, and this mandate will extend to all field players in boys' lacrosse in 2022.
The best chance for survival after cardiac arrest in commotio cordis is with prompt recognition of sudden collapse after chest impact and the immediate activation of the EAP, initiation of CPR and early defibrillation with an onsite AED.11 Pulse checks may be unreliable and agonal breathing or seizure like activity may lead to misdiagnosis so lifesaving treatment with CPR/AED should not be delayed. The greatest chance of survival in commotio cordis is with rapid defibrillation as every minute of delay in delivering a defibrillation shock reduces the chances of survival by 7-10%.12 Research has shown that survival rates are 35% greater in schools with an established EAP and 30% greater if lay responders perform early defibrillation using an onsite AED compared to having to wait for an offsite AED.13,14
The athlete had an unrevealing comprehensive cardiovascular evaluation which included an electrocardiogram with normal QT/QTc intervals, echocardiogram, cardiac magnetic resonance imaging (MRI), maximal effort treadmill stress testing, and ambulatory rhythm monitoring, as per published recommendations.15 Preliminary animal data suggesting an individual susceptibility to commotio cordis was reviewed with the athlete and family but ultimately given his reassuring work up and overall low likelihood for a second event, he was cleared to return to play.16 He wears a NOCSAE approved chest protector and his return has been without incident.
References
- Maron BJ, Poliac LC, Kaplan JA, Mueller FO. Blunt impact to the chest leading to sudden death from cardiac arrest during sports activities. N Engl J Med 1995;333:337-42.
- Maron BJ, Gohman TE, Kyle SB, Estes NAM 3rd, Link MS. Clinical profile and spectrum of commotio cordis. JAMA 2002;287:1142-46.
- Maron BJ, Ahluwalia A, Haas TS, Semsarian C, Link MS, Estes NAM 3rd. Global epidemiology and demographics of commotio cordis. Heart Rhythm 2011;8:1969-71.
- Link MS. Commotio cordis: ventricular fibrillation triggered by chest impact-induced abnormalities in repolarization. Circ Arrhythm Electrophysiol 2012;5:425-32.
- Link MS. Pathophysiology, prevention, and treatment of commotio cordis. Curr Cardiol Rep 2014;16:495.
- Maron BJ, Estes NAM 3rd. Commotio cordis. N Engl J Med 2010;362:917-27.
- Link MS, Wang PJ, Pandian NG, et al. An experimental model of sudden death due to low-energy chest-wall impact (commotio cordis). N Engl J Med 1998;338:1805-11.
- Link MS, Maron BJ, Wang PJ, VanderBrink BA, Zhu W, Estes NAM 3rd. Upper and lower limits of vulnerability to sudden arrhythmic death with chest-wall impact (commotio cordis). J Am Coll Cardiol 2003;41:99-104.
- Link MS, Maron BJ, VanderBrink BA, et al. Impact directly over the cardiac silhouette is necessary to produce ventricular fibrillation in an experimental model of commotio cordis. J Am Coll Cardiol 2001;37:649-54.
- Weinstock J, Maron BJ, Song C, Mane PP, Estes NAM 3rd, Link MS. Failure of commercially available chest wall protectors to prevent sudden cardiac death induced by chest wall blows in an experimental model of commotio cordis. Pediatrics 2006;117:e656-62.
- Drezner JA, Courson RW, Roberts WO, et al. Inter-association task force recommendations on emergency preparedness and management of sudden cardiac arrest in high school and college athletic programs: a consensus statement. Prehosp Emerg Care 2007;11:253-71.
- Link MS, Maron BJ, Stickney RE, et al. Automated external defibrillator arrhythmia detection in a model of cardiac arrest due to commotio cordis. J Cardiovasc Electrophysiol 2003;14:83-87.
- Drezner JA, Rao AL, Heistand J, Bloomingdale MK, Harmon KG. Effectiveness of emergency response planning for sudden cardiac arrest in United States high schools with automated external defibrillators. Circulation 2009;120:518-25.
- Drezner JA, Toresdahl BG, Rao AL, Huszti E, Harmon KG. Outcomes from sudden cardiac arrest in US high schools: a 2-year prospective study from the National Registry for AED Use in Sports. Br J Sports Med 2013;47:1179-83.
- Link MS, Estes NAM 3rd, Maron BJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: Task Force 13: commotio cordis: a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015;66:2439-43.
- Alsheikh-Ali AA, Madias C, Supran S, Link MS. Marked variability in susceptibility to ventricular fibrillation in an experimental commotio cordis model. Circulation 2010;122:2499-504.