Editor's Note: This ECG of the Month was adapted from a JACC: Case Reports ECG Challenge. You can access the original articlehere.
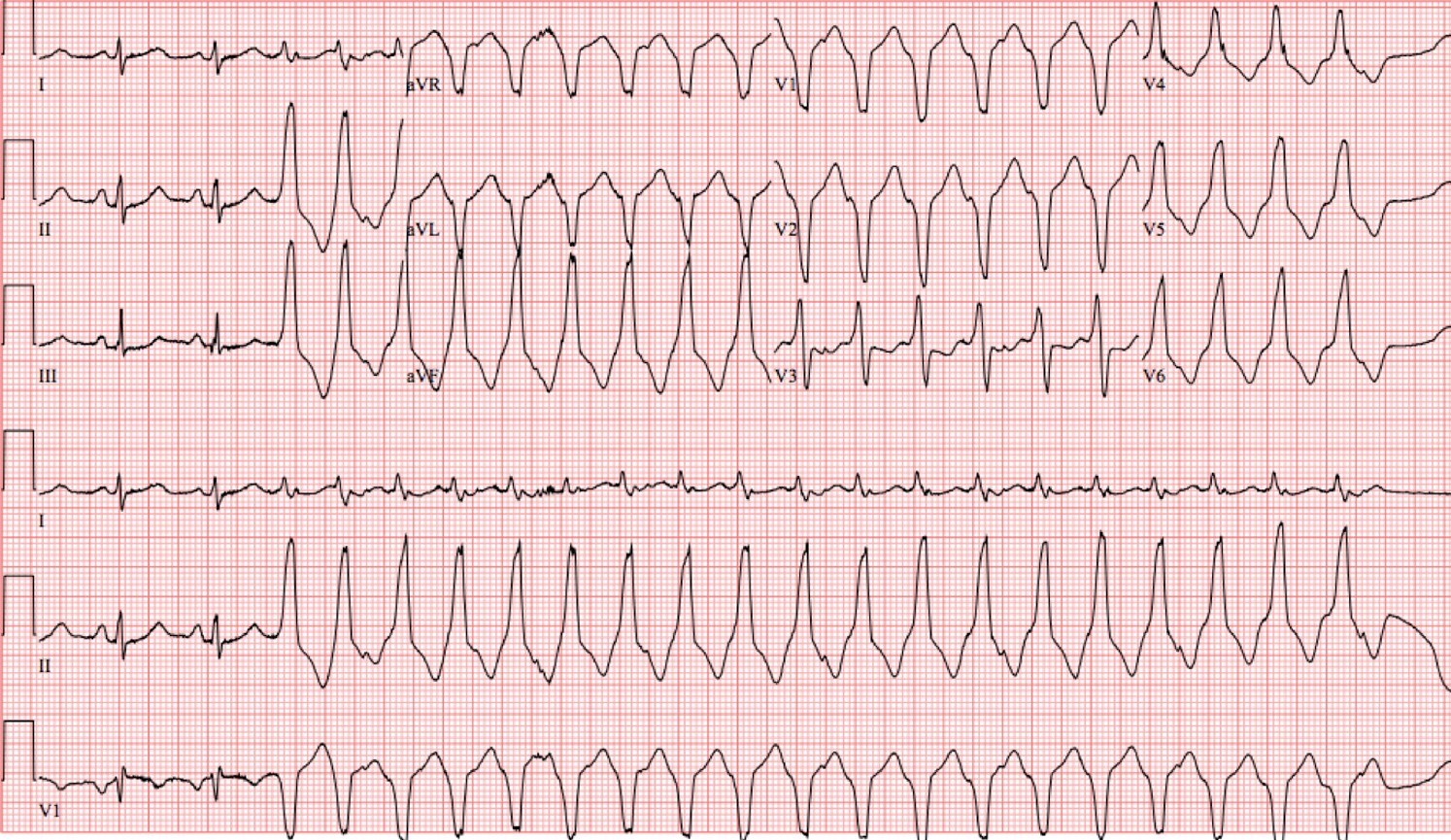
A 27-year-old woman with a history of anxiety presented with several days of intermittent palpitations. She had recently recovered from an upper respiratory infection. On presentation to the emergency department, she had a heart rate of 80 beats/min and blood pressure of 155/78 mm Hg. She had no family history of sudden cardiac death and a normal echocardiogram result. On telemetry, she was noted to have short runs of non-sustained wide complex tachycardia. An electrocardiogram was obtained (Figure 1).
Figure 1: Electrocardiographic Tracing
Figure 1
Which of the following is the correct diagnosis?
Show Answer
The correct answer is: D. Outflow tract ventricular tachycardia.
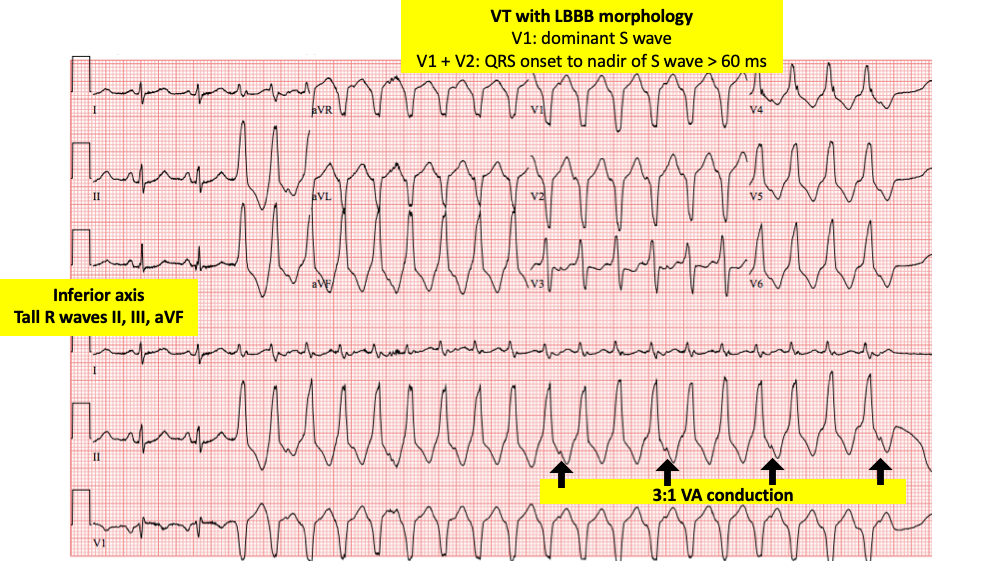
The electrocardiogram (ECG) begins with two beats of sinus rhythm with a heart rate of 91 beats/min, followed by a 19-beat run of a wide complex tachycardia with an inferior axis and left bundle branch block (LBBB) morphology (Figure 2).
Figure 2: ECG Tracing Explained
Figure 2
The differential diagnosis for a wide complex tachycardia includes ventricular tachycardia (VT), supraventricular tachycardia (SVT) with aberrancy, and SVT with pre-excitation. Ventriculo-atrial (VA) dissociation or VA conduction with variable block suggests VT over an SVT. The ECG shown above (Figure 2) shows 3:1 VA conduction, which demonstrates a P wave following every third QRS complex of the tachycardia and the constant relationship between the QRS complex and p-wave. The duration of >60 ms from the onset of the QRS to the nadir of the S wave in V1 and V2 also favors VT over an SVT.1 The LBBB morphology with an inferior axis localizes the origin of the VT most likely to the ventricular outflow tract.
Outflow tract VT is an idiopathic VT which can occur in otherwise healthy individuals at any age without obvious structural heart disease.2 This arrhythmia can arise from either the right ventricular outflow tract (RVOT) or left ventricular outflow tract (LVOT). Conventionally, an earlier R wave transition (i.e., lead V2) favors left ventricular origin, but often this can only be confirmed with mapping in the electrophysiology laboratory. The rightward axis of the RVOT VT occurs because the outflow tracts cross, which renders the RVOT to the left of the LVOT. Outflow tract ventricular tachycardias are caused by cyclic adenosine monophosphate-mediated triggered activity which can be terminated with adenosine.2,3
Treatment of RVOT VT can be deferred if the patient is asymptomatic and has infrequent ectopy unlikely to cause tachyarrhythmia-induced cardiomyopathy. These patients should be monitored for ectopic burden and left ventricular ejection fraction. When treatment is pursued, catheter ablation often is the recommended therapy over metoprolol or propafenone due to the effectiveness and low complication rates of the procedure.4 RVOT VT can be difficult to differentiate from arrhythmogenic right ventricular cardiomyopathy (ARVC),4 and it is important to assess patients for characteristics suggestive of ARVC (e.g., epsilon waves and T wave inversions in V1 to V3) and a family history of sudden cardiac death.
Fascicular VT (answer choice E) is another type of idiopathic VT, although its typical pattern is a right bundle branch block (RBBB) morphology with superior axis when arising from the left posterior fascicle and inferior when arising from the left anterior fascicle.5 The first-line pharmacologic treatment for fascicular VT is verapamil. Moderator band VT (answer choice C) is a macro-re-entrant circuit which arises from the moderator band connecting the right ventricular free wall and the interventricular septum. It is characterized by an LBBB morphology with a superior axis. Moderator band VT can instigate ventricular fibrillation and is often treated with antiarrhythmic agents or ablation.4
This patient was started on verapamil therapy, although she continued to be symptomatic from her ventricular tachycardia. She was brought to the electrophysiology laboratory where her VT was mapped to the RVOT and was successfully ablated with significant improvement in her symptoms.
References
Kindwall KE, Brown J, Josephson ME. Electrocardiographic criteria for ventricular tachycardia in a wide complex left bundle branch block morphology tachycardias. Am J Cardiol 1998;61:1279-83.
Buxton AE, Waxman HL, Marchlinski FE, et al. Right ventricular tachycardia: clinical and electrophysiologic characteristics. Circulation 1983;68:917-27.
Lerman BB. Mechanism, diagnosis, and treatment of outflow tract tachycardia. Nat Rev Cardiol 2015;12:597-608.
Cronin EM, Bogun FM, Maury P, et al. 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias. Heart Rhythm 2020;17:e2-154.
Josephson ME, Callans DJ. Using the twelve-lead electrocardiogram to localize the site of origin of ventricular tachycardia. Heart Rhythm 2005;2:443-6.