Editor's Note: This ECG of the Month was adapted from a JACC: Case Reports ECG Challenge. You can access the original articlehere.
A 66-year-old African-American woman with a 10-year history of sarcoidosis and hypertension presented with progressively worsening exertional dyspnea and fatigue for the past month (Figure 1).
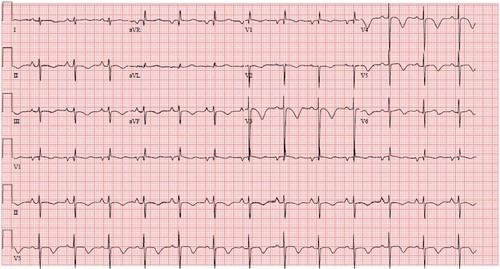
Figure 1: Diagnostic Electrocardiogram
Figure 1
Which clinical diagnosis is most closely represented in this electrocardiogram?
Show Answer
The correct answer is: B. Pulmonary heart disease
The S1S2S3 pattern has had variable criteria for identifying RV dysfunction and pulmonary disease since its initial description in 1960 by Burch and De Pasquale in association with ventricular septal defect and shortly thereafter in adults with chronic obstructive pulmonary disease.1,2 General criteria for this pattern is a predominant S wave deflection in leads I to III usually with right-axis deviation. RV hypertrophy with pulmonary hypertension produces right-dominant forces on a 12-lead electrocardiogram (ECG): a tall R wave in lead V1 (R:S >1); deep S waves in the left precordial leads V5 and V6 (R:S <1); QRS interval <120 ms; right atrial enlargement (P wave in lead II >2.5 mm); and in our case, extreme right-axis deviation. The RV strain pattern, seen here as T wave inversion (TWI) in the anterior and inferior leads, can be mistaken for coronary disease. Apical hypertrophic cardiomyopathy can manifest as deep precordial and high-lateral TWI, high precordial voltages, and left atrial enlargement. Arrhythmogenic RV cardiomyopathy can show ε waves, QRS fragmentation, and right precordial lead QRS prolongation with a delayed S-wave terminal deflection. Various constellations of these criteria for RV hypertrophy and pulmonary heart disease, which typically include S1S2S3, and have shown a diagnostic sensitivity of <50% and specificity of >95%, suggesting ECG to be a powerful modality in patients with an elevated clinical suspicion for pulmonary pathology.3
This patient's subsequent echocardiogram (Figure 2) showing RV hypertrophy and dilatation, and the chest x-ray (Figure 3) shows stage 4 sarcoidosis with lung fibrosis, which supports the ECG findings.
Figure 3: Chest X-Ray Showing Severe Interstitial Fibrosis Secondary to End-Stage Pulmonary Sarcoidosis
Figure 3
References
Burch GE and DePasquale N. The electrocardiogram, spatial vectorcardiogram, and ventricular gradient in congenital ventricular septal defect. Am Heart J 1960;60:195-211.
Pryor R. The S1, S2, S3 syndrome in chronic pulmonary disease. Dis Chest 1964;46:226.
Lehtonen J, Sutinen S, Ikaheimo M, and Paakko P. Electrocardiographic criteria for the diagnosis of right ventricular hypertrophy verified at autopsy. Chest 1988;93:839-42.