A 58-year-old man with a past medical history of type 2 diabetes mellitus (T2DM), hypertension, dyslipidemia, was brought to our emergency department with 1 week of pleuritic chest pain, shortness of breath, palpitations, and presyncope. His home medications included ramipril, atorvastatin, metformin, and gliclazide. He was initially seen in a community-based hospital where he was found to have an elevated D-dimer and underwent computed tomography (CT) chest that showed a small pericardial effusion, and no evidence of pulmonary embolism. His cardiac enzymes and electrocardiograms (ECG) were normal, and thus he was discharged home. He continued to be symptomatic with worsening shortness of breath, palpitations, and presyncope that prompted him to visit our quaternary care center's emergency department.
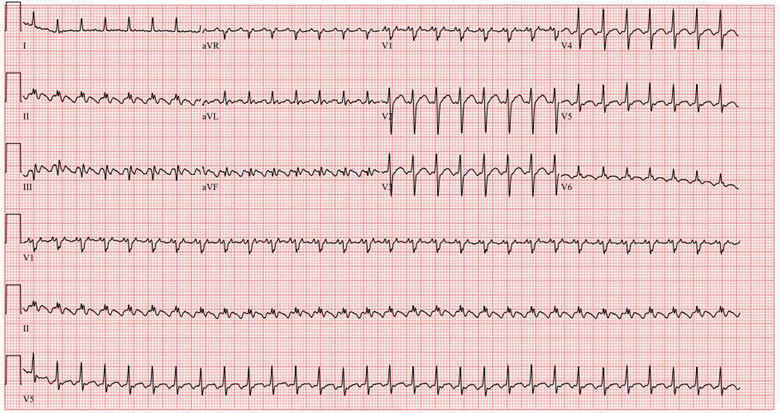
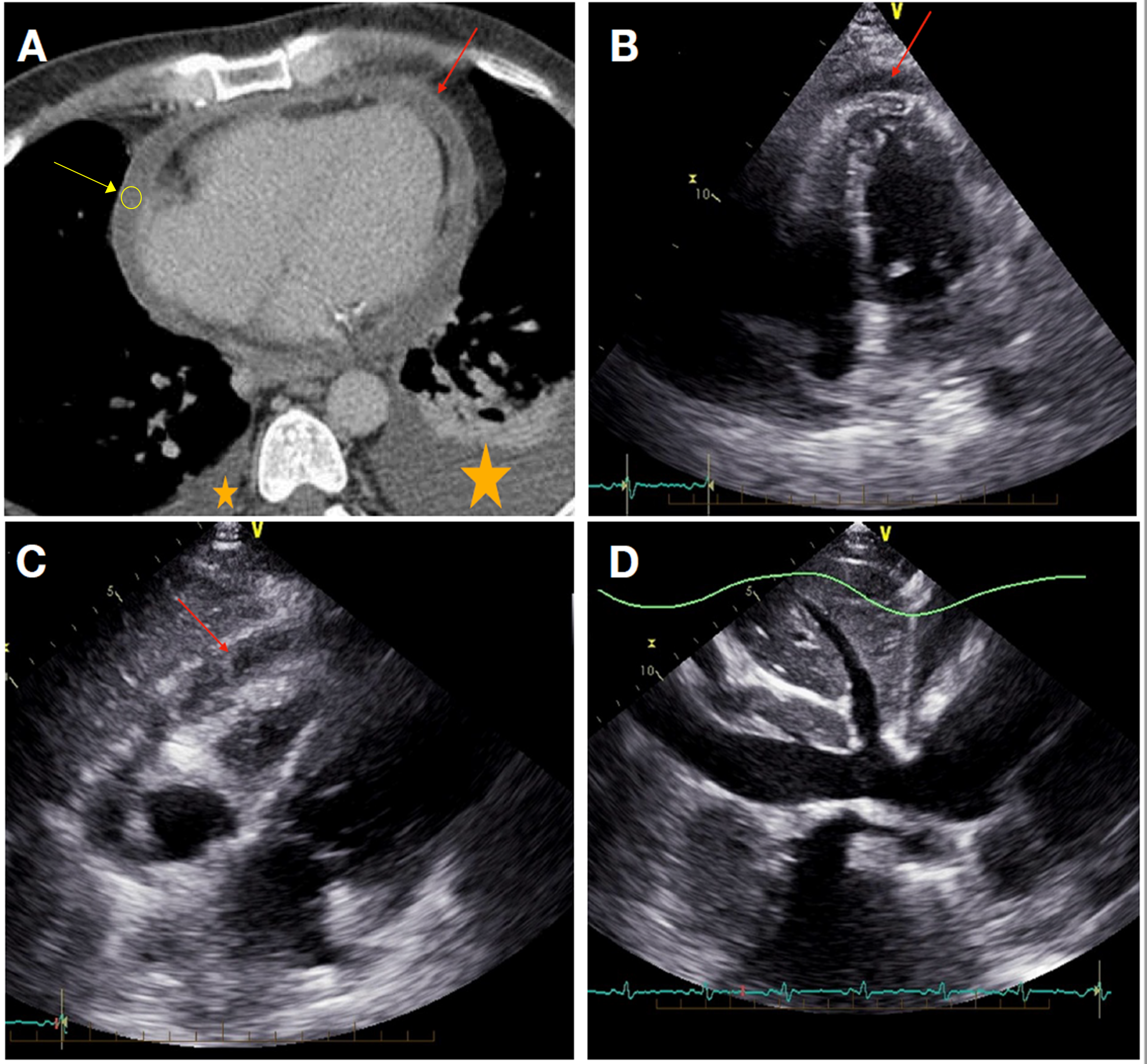
On arrival to our institution, the patient was found to be in new atrial flutter (ventricular rates of 160-180 BPM), his blood pressure was 109/69 mmHg and he was hemodynamically stable, and afebrile. His oxygen saturation was 98% on room air. The cardiopulmonary exam revealed normal jugular venous pressure (JVP), distant heart sounds (no pericardial friction rub), and reduced air entry bilaterally with dullness on percussion. His abdominal exam was unremarkable. His ECG demonstrated atrial flutter with 2:1 atrioventricular (AV) conduction (Figure 1). He had a repeat CT chest which demonstrated increased size of the pericardial effusion to now moderate sized with a CT attenuation value of 11 Hounsfield units (HU) for the pericardial fluid, new small to moderate bilateral pleural effusions, and pericardial enhancement suggestive of acute pericarditis (Figure 2A).
Initial laboratory workup at our institution revealed leukocytosis with a white blood cell (WBC) count 15.5 10^9/L (normal 4.50-11.00), neutrophile predominant with neutrophils at 87% (normal 40-70%), anemia with hemoglobin (Hb) of 106 g/L (normal 135-175) and a normal platelet count, mildly elevated transaminase with alanine aminotransferase (ALT) of 59 U/L (normal 6-45) with normal aspartate aminotransferase (AST), total bilirubin and coagulation profile. His C-reactive protein (CRP) was elevated at 279.94 mg/L (normal 0.00-5.00). His high sensitivity troponin I (HSTnI) was 47.5 ng/L (normal <= 17.5).
A transthoracic echocardiogram (TTE) showed normal left ventricular (LV) size and function with no regional wall motion abnormalities and normal right ventricular (RV) size and function. Right atrial (RA) pressure was estimated at 15 mmHg. A small to moderate circumferential pericardial effusion (most pronounced anterior to RV free wall, 13 mm) with mixed echogenicity and fibrinous stranding was identified. A septal bounce with some lateral apical tethering was also noted without interventricular dependence. Overall, in the presence of a plethoric inferior vena cava (IVC), early constrictive physiology was suggested (Figure 2B-D).
His course in hospital/illness was complicated with hypotension in the context of the increased size of the pericardial effusion, requiring an urgent subxiphoid pericardial window and pericardial drain. His pericardial fluid was negative for any infectious or malignant cause and a pericardial biopsy demonstrated acute fibrinous pericarditis suggestive of infectious or reactive pericarditis. He was treated with prednisone 30 mg daily in addition to colchicine 0.6 mg twice daily with clinical improvement and a drop in CRP from 279.8 to 17.3. A follow-up TTE a few days later demonstrated no significant residual pericardial effusion. His subsequent autoimmune and malignancy workup was negative. In terms of his atrial flutter, he was started on intravenous (IV) amiodarone during his hypotensive episode, but his heart rate ultimately improved post pericardiocentesis; and was maintained on metoprolol and amiodarone for consideration of outpatient elective ablation once out of the acute phase of his pericardial disease. Anticoagulation was initiated with IV heparin after the pericardial drain was removed and he was eventually transitioned to apixaban. He had a repeat echocardiogram prior to discharge to ensure no hemorrhagic transformation of the pericarditis. He was discharged in a stable condition, symptom-free with a prednisone taper schedule.
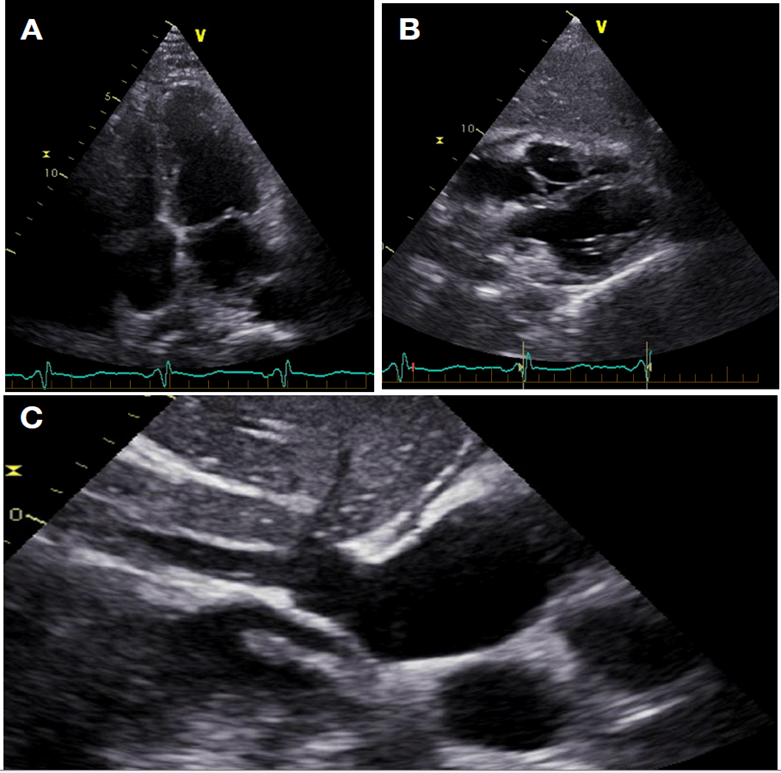
He remained symptom-free until approximately 6 weeks later, once his prednisone dose was at 10 mg daily as per his taper, when he developed recurrent symptoms of pleuritic chest pain and palpitations. A repeat CT chest demonstrated moderate-sized pericardial effusion and a repeat TTE demonstrated a small circumferential pericardial effusion approximately 3 mm with subtle interventricular dependence and a septal bounce with strain reversus, but no annular reversus with overall no evidence of constrictive physiology (Figure 3). His CRP was elevated again at 181.49, his prednisone dose was increased to 20 mg daily with clinical improvement and improvement in inflammatory markers.
Figure 1
Figure 1
Figure 1: ECG demonstrating atrial flutter with 2:1 conduction.
Figure 1: ECG demonstrating atrial flutter with 2:1 conduction.
Figure 2
Figure 2
Figure 2: (A) CT Chest demonstrating pericardial enhancement with moderate sized circumferential pericardial effusion (red arrow) with a CT attenuation value of 11 HU (yellow arrow) and bilateral pleural effusions (yellow stars). (B) Apical 4-chamber TTE demonstrating moderate circumferential pericardial effusion with mixed echogenicity and fibrinous stranding (red arrow). (C) Subcostal 4-Chamber TTE again, demonstrating moderate pericardial effusion most pronounced anterior the RV free wall (red arrow). (D) IVC view showing a plethoric IVC which was not collapsible.
Figure 2: (A) CT Chest demonstrating pericardial enhancement with moderate sized circumferential pericardial effusion (red arrow) with a CT attenuation value of 11 HU (yellow arrow) and bilateral pleural effusions (yellow stars). (B) Apical 4-chamber TTE demonstrating moderate circumferential pericardial effusion with mixed echogenicity and fibrinous stranding (red arrow). (C) Subcostal 4-Chamber TTE again, demonstrating moderate pericardial effusion most pronounced anterior the RV free wall (red arrow). (D) IVC view showing a plethoric IVC which was not collapsible.
Figure 3
Figure 3
Figure 3: (A) Apical 4-chamber TTE demonstrating small (~3mm) circumferential pericardial effusion. (B) Subcostal 4-chamber TTE demonstrating a small pericardial effusion most pronounced near the anterior atrioventricular groove. (C) IVC view showing a small IVC, no longer plethoric, and it was collapsible.
Figure 3: (A) Apical 4-chamber TTE demonstrating small (~3mm) circumferential pericardial effusion. (B) Subcostal 4-chamber TTE demonstrating a small pericardial effusion most pronounced near the anterior atrioventricular groove. (C) IVC view showing a small IVC, no longer plethoric, and it was collapsible.
If the patient develops further recurrence of his pericarditis despite steroid and colchicine, what would be the next best method for treatment?
Show Answer
The correct answer is: C. Biologic therapy (anakinra/rilonacept)
Discussion:
The patient had incessant pericarditis with a resurgence of symptoms in the context of a steroid taper. Incessant pericarditis is an episode of pericarditis lasting >4-6 weeks but <3 months without remission. Recurrent pericarditis is diagnosed with a documented first episode of acute pericarditis, a symptom-free interval of at least 4-6 weeks, and evidence of recurrence of the pericarditis. The criteria used for the diagnosis of recurrent pericarditis is the same as acute pericarditis with at least two of the four following criteria: pericarditic chest pain, pericardial rubs, ECG demonstrating diffuse ST-elevations or PR depressions, new or worsening pericardial effusion. Recurrent pericarditis affects 15-30% of patients and up to 50% of patients not treated with colchicine.1
Whether it be a primo diagnosis or a resurgence of symptoms, TTE is considered the first-line imaging test in patients with suspected pericardial disease due to its accurate detection of pericardial fluid, cardiac tamponade, any myocardial involvement with ventricular dysfunction.2 Nonetheless, advanced imaging such as cardiac CT may provide supportive and confirmatory findings to support the diagnosis in atypical or doubtful cases such as in therapeutic difficulties, or pericarditis associated with specific diseases (e.g., neoplasm).3-4 CT is the most accurate technique to image calcified tissue and to provide excellent anatomical detail of the heart and pericardium.3 Cardiac CT demonstrates pericardial inflammation through evidence of pericardial thickening, edema, and contrast enhancement of the pericardium.1,3 It also has the added advantage of accurately localizing and characterizing the fluid by measuring the CT attenuation using Hounsfield units (HU). HU of <10 units suggest transudative effusions with CT attenuation similar to that of water, while HU above 10 units suggest exudative fluid with high protein content. CT attenuations ranging from 20 to 60 HU suggest exudative fluid which is more purulent, malignant, or myxedematous in nature, while an attenuation ˃60 HU is more suggestive of a hemorrhagic effusion.3 Findings of recurrent pericarditis on CT chest are like that of acute pericarditis with thickened pericardial layers with enhancement when contrast is applied, a variable amount of pericardial fluid with intrapericardial fibrinous strands. There could be heterogeneous distributions due to fibrotic adhesions and irregular pericardial delineation.1,3,4
Treatment of refractory pericarditis should be targeted at the underlying cause. In cases of incomplete response to aspirin or NSAIDs or a contraindication/intolerance to it (as in this case with therapeutic anticoagulation), then corticosteroids at low to moderate doses can be added (after ruling out infection, especially bacterial and tuberculosis) in addition to colchicine (triple therapy) to achieve better control of symptoms.1,5 Tapering of corticosteroids should only be done after a complete response, and taper should be slow and attempted only if symptoms are absent and CRP is normal.1 It should be kept in mind that below a certain dosage (typically ~15 mg of prednisone daily) re-emergence of symptoms could occur.5
For those who require long-term high doses of corticosteroids or those who are unresponsive to steroids despite NSAIDs and colchicine, several drugs have been used as third-line options in cases of proven infection-negative, recurrent pericarditis including azathioprine, IVIG, anakinra, and rilonacept.1 The first option given is incorrect because our patient was started on apixaban for anticoagulation for his atrial flutter and adding additional NSAIDs would increase his risk for bleeding. Azathioprine is mainly useful as a long-term corticosteroid-sparing agent and not in the acute phase, thus less helpful in our case. Anakinra is more effective during the acute phase.1 Anakinra is a recombinant human interleukin 1 (IL-1) receptor antagonist (IL-1ra), that competes and blocks the IL-1 receptor counteracting an inflammatory response.6 It has been shown that it is a very effective drug for treating recurrent pericarditis with low recurrence rates at full doses. However, recurrence rates are considerably high during the tapering phase or after discontinuation.6,7 Rilonacept is another biologic agent, which acts as an interleukin-1α and interleukin-1β cytokine trap, and has also been shown to have a rapid clinical response in cases of recurrent pericarditis and could be weaned from other therapy, including glucocorticoids.8 Pericardiectomy may be considered only after a thorough unsuccessful attempt of medical therapy and has been demonstrated to be a safe and effective method in patients in whom medical management has failed.1,9 In our case, not all medical treatments have been exhausted, thus pericardiectomy is not the correct answer. Thus, in our case, the most appropriate answer would be to start a biologic agent (anakinra or rilonacept) in case of further recurrence despite steroids and colchicine.
Anticoagulation in acute pericarditis is an area that needs to be studied in more detail with no American guidelines addressing this issue. The European guidelines for the diagnosis and management of pericardial diseases suggest that the use of anticoagulation in acute pericarditis is a minor risk factor for poor prognosis and should be avoided in uremic or iatrogenic pericarditis, but may be considered safe in other causes.1 In one multivariable analysis of 453 patients with acute pericarditis, the use of anticoagulation was not associated with an increased risk of complications.10 In clinical practice, it is reasonable to admit such patients to monitor clinically in the first few days.
Back to the case, due to recurrence, despite prednisone and colchicine, our patient was subsequently started on anakinra 100 mg/day subcutaneously and was tapered off steroids. His symptoms resolved, inflammatory markers normalized, and he remained asymptomatic on further follow-up.
References
Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) Endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J 2015;36:2921-64.
Cosyns B, Plein S, Nihoyanopoulos P, et al. European Association of Cardiovascular Imaging (EACVI) position paper: multimodality imaging in pericardial disease. Eur Heart J Cardiovasc Imaging 2015;16:12-31.
Chetrit M, Xu B, Verma BR, Klein AL. Multimodality imaging for the assessment of pericardial diseases. Curr Cardiol Rep 2019;21:41
Fadl SA, Nasrullah A, Harris A, Edwards R, Kicska G. Comprehensive review of pericardial diseases using different imaging modalities. Int J Cardiovasc Imaging 2020;36:947-69.
Lilly LS. Treatment of acute and recurrent idiopathic pericarditis. Circulation 2013;127:1723-26.
de Oliveira Correia ET, dos Santos Barbetta LM, Latini de Almeida JPC, Mesquita ET. Anakinra in recurrent pericarditis: current evidence on clinical use, effectiveness, and safety. J Cardiovasc Pharmacol 2020;76:42-49.
Lazaros G, Imazio M, Brucato A, et al. Anakinra: an emerging option for refractory idiopathic recurrent pericarditis: a systematic review of published evidence. J Cardiovasc Med (Hagerstown) 2016;17:256-62.
Klein AL, Imazio M, Cremer P, et al. Phase 3 trial of interleukin-1 trap rilonacept in recurrent pericarditis. NEngl J Med 2021;384:31-41.
Khandaker MH, Schaff HV, Greason KL, et al. Pericardiectomy vs medical management in patients with relapsing pericarditis. Mayo Clin Proc 2012;87:1062-70.
Imazio M, Cecchi E, Demichelis B, et al. Indicators of poor prognosis of acute pericarditis. Circulation 2007;115:2739-44.