A 22-year-old male with past medical history of Coxsackie myocarditis in 2019 presented to the emergency department with acute chest pressure and diaphoresis. He described his chest pain as squeezing with radiation to the back. The patient denied dyspnea, edema, and lightheadedness. Physical examination and vital signs were within normal limits. Cardiovascular exam showed regular rate, normal rhythm, S1, S2 sounds, and no pericardial rub. He was taking no medications and had received his second dose of the Pfizer (BNT162b2) mRNA Coronavirus-19 disease (COVID-19) vaccine 3 days prior to symptoms onset.
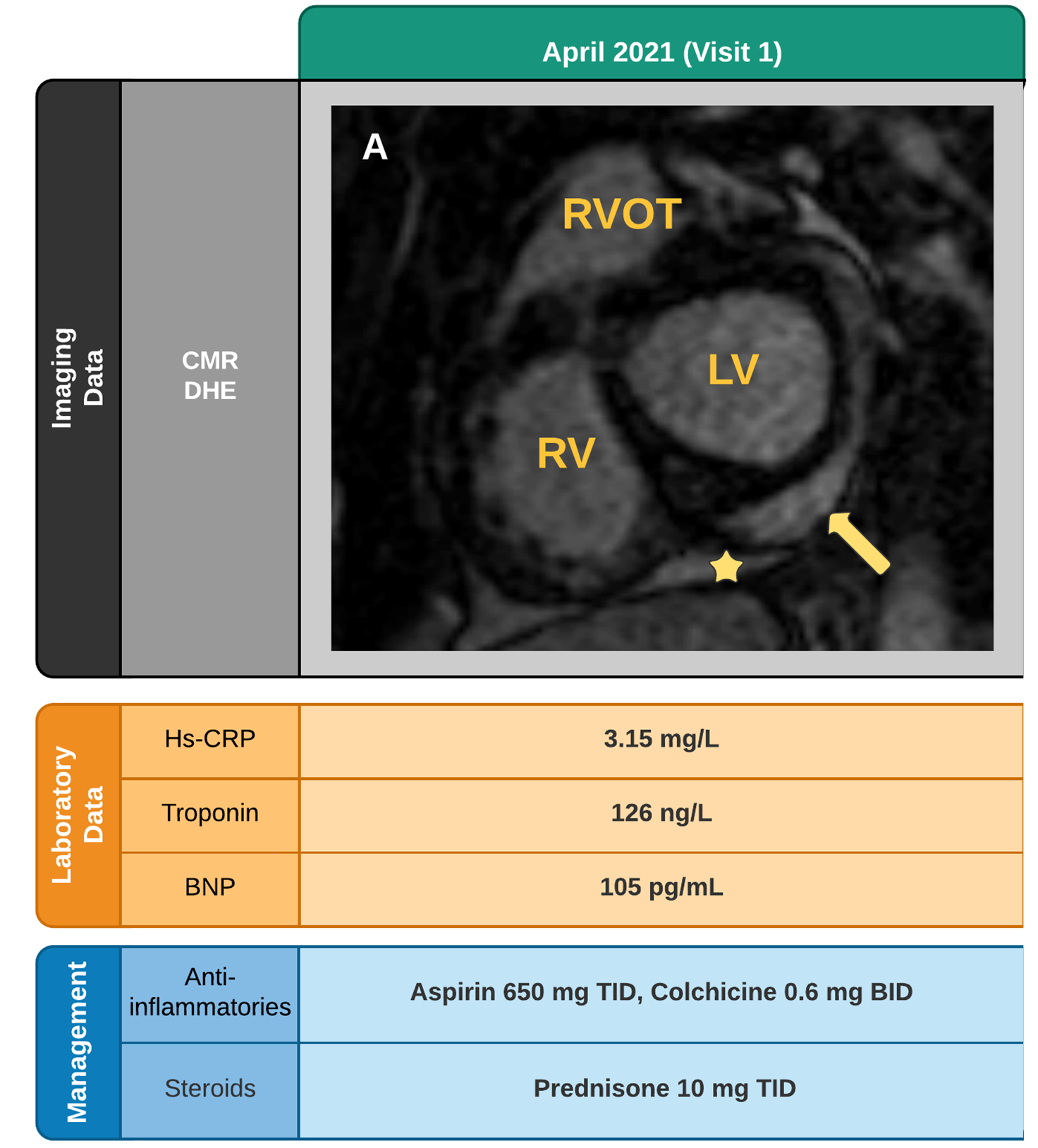
Laboratory examination showed high sensitivity C-reactive protein (hs-CRP) (3.15 mg/L), high-sensitivity troponin T (126 ng/mL) and brain natriuretic peptide (105 pg/mL) levels were all elevated. Severe acute respiratory syndrome-Coronavirus-2 (SARS-CoV-2) IgG test was positive indicative of prior infection or prior vaccination status. Electrocardiogram (ECG) showed diffuse ST-segment elevation suggestive of pericarditis. Chest x-ray (CXR) was negative. Bedside echocardiography (echo) demonstrated mildly reduced ejection fraction (EF) (45%). In our patient, cardiac magnetic resonance imaging (CMR) identified a small pericardial effusion, and profound basal inferolateral and lateral myocardial involvement (Figure 1A).
Figure 1A: Timeline of Disease Course
Figure 1A
A. Initial CMR with basal inferolateral and lateral myocardial involvement (arrows) and associated pericardial effusion (star). BNP: Brain Natriuretic Peptide; CMR: Cardiac Magnetic Resonance Imaging; DHE: Delayed Enhancement; Hs-CRP: High Sensitivity C - reactive protein; LV: Left Ventricle; RV: Right Ventricle; RV: Right Ventricle Outflow Tract
A. Initial CMR with basal inferolateral and lateral myocardial involvement (arrows) and associated pericardial effusion (star). BNP: Brain Natriuretic Peptide; CMR: Cardiac Magnetic Resonance Imaging; DHE: Delayed Enhancement; Hs-CRP: High Sensitivity C - reactive protein; LV: Left Ventricle; RV: Right Ventricle; RV: Right Ventricle Outflow Tract
Given his clinical and imaging findings, he was diagnosed with perimyocarditis secondary to COVID-19 vaccination. He was prescribed aspirin 650 mg TID and colchicine 0.6 mg BID. Unfortunately, he discontinued aspirin therapy due to gastrointestinal distress. He was then given a 1-month prednisone taper (30 mg). At 6-week follow-up, the patient noted his pain was significantly improved. The patient had completed his steroid taper and laboratory markers and ECG were normal. Echo showed EF recovery without the presence of a pericardial effusion.
What is the best step in management to assess for improvement in perimyocardial inflammation?
Show Answer
The correct answer is: A. CMR imaging
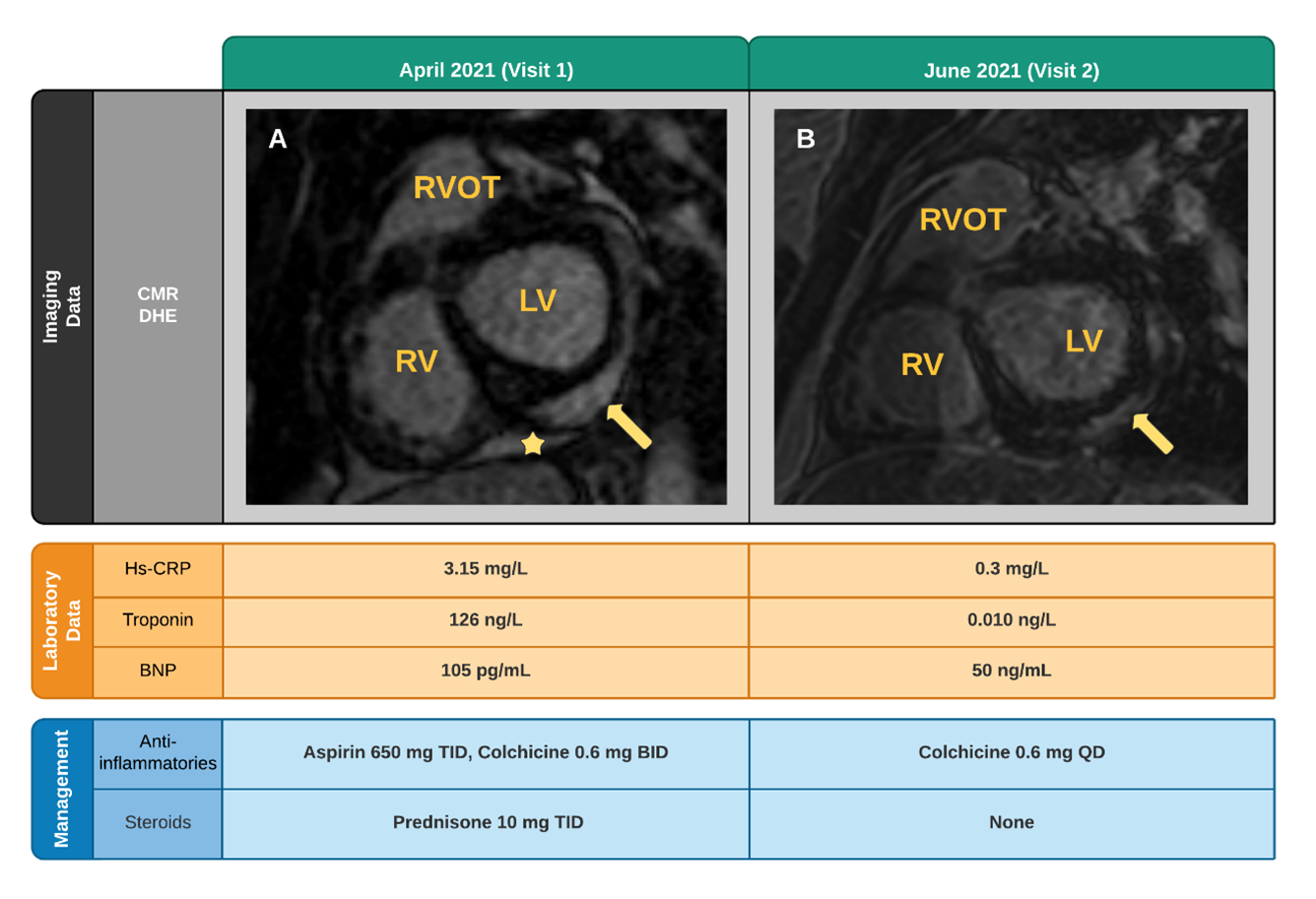
Repeat CMR demonstrated interval improvement in pericardial effusion and delayed enhancement (Figure 1B). His colchicine was tapered to 0.6 mg daily and he was told to follow up in 4 months.
Figure 1B: Timeline of Disease Course
Figure 1B
A. Initial CMR with basal inferolateral and lateral myocardial involvement (arrows) and associated pericardial effusion (star).
B. Follow up CMR with interval improvement in pericardial effusion and delayed enhancement (arrows).
A. Initial CMR with basal inferolateral and lateral myocardial involvement (arrows) and associated pericardial effusion (star).
B. Follow up CMR with interval improvement in pericardial effusion and delayed enhancement (arrows).
COVID-19 vaccination efforts have been increasing, resulting in many receiving mRNA vaccines. The COVID-19 mRNA vaccine encodes for the spike glycoprotein of the virus. The vaccine's liquid suspension particles allow for direct delivery of mRNA into host cells. Once intracellular, the mRNA upregulates ribosomal activity to create the spike glycoprotein.1 The spike glycoprotein is then presented on the surface of the cell; this subsequently triggers the immune system to produce antibodies specific to the spike protein.1,2 COVID-19 vaccine side effects are typically mild and may involve local injection site pain, myalgia, and fatigue. Serious adverse effects are rare, but recent reports have suggested that mRNA COVID-19 vaccines may cause myocarditis, pericarditis, and myopericarditis. As of June 11th 2021, the Centers for Disease Control (CDC) have identified 323 cases of myocarditis, pericarditis, and myopericarditis in the United States.3
CDC findings suggest that afflicted patients are more likely to be male, younger with a median age of 19 years, and experience symptoms within 2 days after vaccination.3 The most common presenting symptoms include chest pain (85%-95%), fever (65%), dyspnea (19%-49%), and syncope (6%).4 The CDC also determined that patients were more likely to be hospitalized, but clinical course was mild as most patients recover fully.3,5 While no consensus mechanism has been elucidated, vaccine component hypersensitivity, inflammatory reaction, and inappropriate immune system activation have been mentioned as potential causes.4
Perimyocarditis diagnosis requires fulfillment of two out of four major criteria: pleuritic chest pain, auscultation of pericardial rub, ECG changes, and effusion on imaging.6 Additionally, patients must also have elevated biomarkers suggestive of myocardial injury (troponin) and reduced left ventricular function.4 Our patient presented with pleuritic chest pain, characteristic ECG changes, effusion on imaging, minor LV dysfunction, and biomarker elevation. Imaging with echo and CMR are useful for diagnosis and informing clinical course. Echo can identify the presence of effusion as well as be used for risk stratification in patients with cardiac tamponade.7 Findings of pericarditis on CMR include T1-weighted enhancement of the thickened pericardium, T2-weighted increased pericardial intensity, and presence of pericardial edema on delayed hyperenhancement (DHE).8 Notably, CMR findings of DHE in patients who develop non-vaccine myocarditis is associated with increased risk of cardiac complications.9 Therefore, assessing the long term risk of complications in patients who have DHE on CMR after vaccination is paramount.9
While much is still unknown about management of perimyocarditis in patients after COVID-19 vaccination, patients are treated using current guidelines for pericarditis management (non-steroidal anti-inflammatory drugs [NSAIDs], colchicine, and/or steroids). Specifically, for our patient steroids were added due to his intolerance towards aspirin therapy. Luckily, our patient was able to achieve clinical improvement on this regimen alone. Biologics (rilonacept) are indicated in patients who develop dependence on NSAIDs, colchicine, and steroids.10
References
Jackson LA, Anderson EJ, Rouphael NG, et al. An mRNA vaccine against SARS-CoV-2 — preliminary report. N Engl J Med 2020;383:1920-31.
Hendaus MA, Jomha FA. mRNA Vaccines for COVID-19: a simple explanation. Qatar Med J 2021;Feb 18;[Epub ahead of print].
Gargano JW, Wallace M, Hadler SC, et al. Use of mRNA COVID-19 vaccine after reports of myocarditis among vaccine recipients: update from the Advisory Committee on Immunization Practices — United States, June 2021. MMWR Morb Mortal Wkly Rep 2021;70:977-82.
Hudson B, Mantooth R, DeLaney M. Myocarditis and pericarditis after vaccination for COVID‐19. J Am Coll Emerg Physicians Open 2021;2:e12498.
Lazaros G, Klein AL, Hatziantoniou S, Tsioufis C, Tsakris A, Anastassopoulou C. The novel platform of mRNA COVID-19 vaccines and myocarditis: clues into the potential underlying mechanism. Vaccine 2021;39:4925-27.
Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J 2015;36:2921-64.
Chetrit M, Xu B, Verma BR, Klein AL. Multimodality imaging for the assessment of pericardial diseases. Curr Cardiol Rep 2019;21:41.
Imazio M, Pivetta E, Palacio Restrepo S, et al. Usefulness of cardiac magnetic resonance for recurrent pericarditis. Am J Cardiol 2020;125:146-51.
Dionne A, Sperotto F, Chamberlain S, et al. Association of myocarditis with BNT162b2 messenger RNA COVID-19 vaccine in a case series of children. JAMA Cardiol 2021;6:1445-50.
Klein AL, Imazio M, Cremer P, et al. Phase 3 trial of interleukin-1 trap rilonacept in recurrent pericarditis. N Engl J Med 2021;384:31-41.