Editor's Note: This ECG of the Month was adapted from a JACC: Case Reports ECG Challenge. You can access the original articlehere.
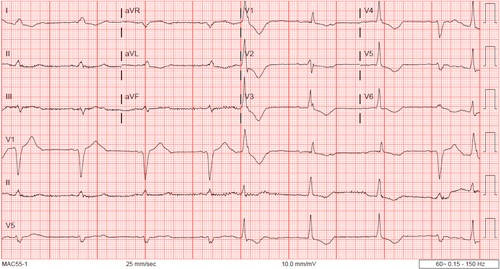
A 72-year-old man with a medical history of coronary artery disease, severe aortic stenosis with mechanical aortic valve replacement, paroxysmal atrial fibrillation, right bundle branch block (RBBB), hypertension, diabetes, obesity, and a recent hip arthroplasty complicated by osteomyelitis on outpatient vancomycin infusions became unresponsive before infusion and was found to be in ventricular fibrillation that required one shock.
An electrocardiogram was obtained (Figure 1)
Figure 1: 12-Lead Electrocardiogram Obtained During Hospitalization
Figure 1
Which of the following is the correct diagnosis?
Show Answer
The correct answer is: C. Normal sinus rhythm with 2:1 atrioventricular block with LBBB and RBBB with occasional PVCs.
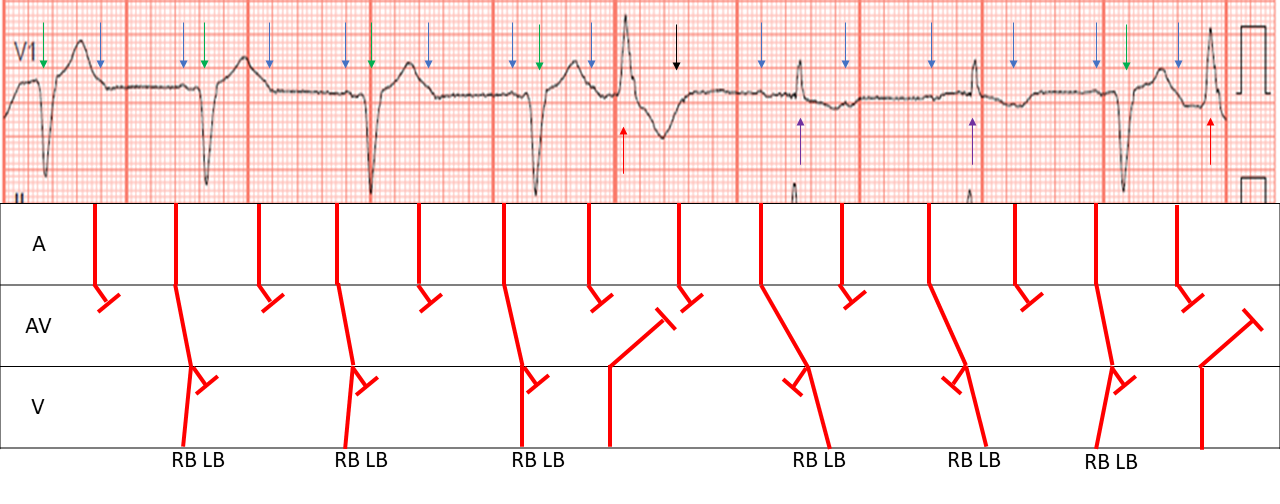
As depicted in the ladder diagram (Figure 2) sinus P waves initially conduct 2:1 in a LBBB pattern, followed by a PVC with a buried P wave. The next P wave conducts with a more prolonged PR interval and a RBBB morphology again with 2:1 conduction. The last conducted P wave then conducts with a shorter PR interval and back to a LBBB morphology followed by another PVC.
Figure 2: Ladder Diagram From Presented ECG
Figure 2
Caption-Caption-Caption
This diagram illustrates the alternating bundle branch blocks and A/V Block. Blue arrows highlight P waves, green arrows QRS complexes, red premature ventricular contractions, and black arrows highlight hidden waves
The phenomenon of alternating bundle branch blocks is well described in the literature as conferring a high risk of progression to complete heart block.1 In this electrocardiogram, there is initial conduction through the right bundle, causing the LBBB appearance that is noted in the first four complexes. A PVC causes the right bundle to then become refractory to conduction (due to retrograde activation), which allows for conduction through the left bundle with a more prolonged PR interval and the RBBB morphology noted in the two complexes that follow the PVC. This demonstrates that, with more time resulting from the post-extra systolic pause, the left bundle is capable of conduction, albeit at an even longer time interval than the right bundle.
Although we believe the previous explanation is the most likely, a similar effect can be noted in the "linking phenomenon," with which a PVC eliminates retrograde concealed penetration of the opposite bundle branch and changes ventricular activation. This is less likely in this case for three reasons: 1) the presence of significant underlying conduction disease (2:1 heart block); 2) inability of the PVC to "peel back" refractoriness and restore normal conduction; and 3) variable PR intervals depending on which bundle branch the impulse travels down.2,3 Another phenomenon that cannot be excluded is that the RBBB beats are fusion beats from left ventricular PVCs.
Coronary angiography did not reveal obstructive coronary artery disease, and cardiac arrest was believed likely secondary to high-grade atrioventricular block and bradycardia with an early after depolarization event triggering ventricular fibrillation. No further ventricular fibrillation was noted, although there was significant ventricular ectopy and a dual-chamber implantable cardioverter-defibrillator was placed for secondary prevention.
References
Stark S, Farshidi A. Mechanism of alternating bundle branch aberrancy with atrial bigeminy: electrocardiographic-electrophysiologic correlates. J Am Coll Cardiol 1985;5:1491-5.
Lehmann MH, Denker S, Mahmud R, Addas A, Akhtar M. Linking: a dynamic electrophysiologic phenomenon in macroreentry circuits. Circulation 1985;71:254-65.
Hillyard J, Mankad P, Ellenbogen KA, Padala SK. Resolution of right bundle branch block after a premature ventricular beat: what is the mechanism? Heart Rhythm Case Rep 2019;5:597-9.