The patient is a 33-year-old male with hypertrophic cardiomyopathy (HCM), congenital perimembranous ventricular septal defect, and hypertension who presents to clinic for consultation of primary prevention implantable cardioverter-defibrillator (ICD). He has a family history of HCM in his mother, sister, and maternal uncle. His maternal uncle experienced sudden cardiac death (SCD) status post ICD placement and subsequently underwent orthotopic heart transplantation. His mother and sister both have an ICD in place. He denies experiencing any chest pain, shortness of breath, paroxysmal nocturnal dyspnea, orthopnea, palpitations, dizziness, lightheadedness, syncope, near syncope, or pedal edema. He is currently prescribed losartan 50mg daily.
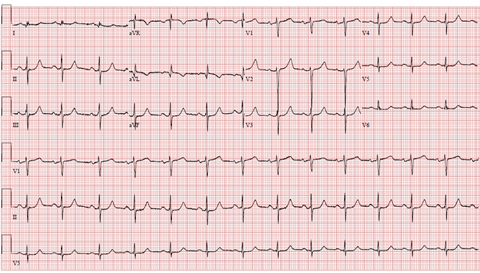
His electrocardiogram (ECG) showed normal sinus rhythm with a heart rate of 80 beats per minute. There is a possible old septal infarction of undetermined age. The QT interval is 406 milliseconds.
Figure 1
Figure 1
A Holter monitor showed 2 premature ventricular contractions (PVCs), 1 premature atrial contraction (PAC), and no arrhythmias.
A transthoracic echocardiogram showed concentric left ventricular hypertrophy (LVH) with septal thickness of 1.5 cm.
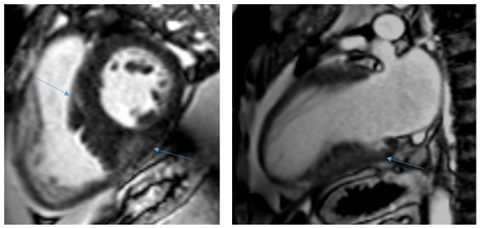
A cardiac magnetic resonance imaging (MRI) showed asymmetric septal hypertrophy (ASH) that was at maximum 2.4 cm without evidence of left ventricular outflow tract (LVOT) obstruction, a small perimembranous ventricular septal defect (VSD), normal biventricular function, and diffuse patchy midwall fibrosis involving more than 15% of the myocardium.
Figure 2a and b
Figure 2
Figure 2a and b: Cardiac MRI short axis and long axis views showing late gadolinium enhanced fibrosis (see arrows).
Figure 2a and b: Cardiac MRI short axis and long axis views showing late gadolinium enhanced fibrosis (see arrows).
What is the most appropriate next step?
Show Answer
The correct answer is: C. Implantation of primary prevention ICD
While genetic testing is helpful to identify family members at risk of developing HCM, the utility of genetic testing for the assessment of sudden cardiac risk is uncertain.
Implantable loop recorder would not likely add value as the patient already underwent a Holter monitor without any arrhythmias detected.
Primary prevention ICD would be recommended given the patient's family history of second degree relative with SCD and extensive fibrosis seen on cardiac MRI. Thus, answer C. is the best possible next step in this case.
No intervention is not appropriate, as sudden cardiac risk evaluation is recommended at initial evaluation and every 1-2 years subsequently. Furthermore, individual clinical judgment and shared decision making is essential for the decision of ICD placement.
For patients with HCM, ICD placement is recommended for secondary prevention in the setting of previously documented cardiac arrest or sustained ventricular tachycardia (Class 1).1 For patients with an uncertain risk for primary prevention of SCD after clinical assessment, cardiac MRI is beneficial to evaluate maximum LV wall thickness, ejection fraction, LV apical aneurysm, and myocardial fibrosis (Class 1).1
ICD placement for primary prevention is reasonable if a patient has more than one of these major risk factors for SCD: family history of sudden death from HCM of ≥1 first-degree or close relatives who are ≥50 years of age, personal history of unexplained, non-vasovagal syncope, massive LVH wall thickness ≥30 mm, LV systolic dysfunction with ejection fraction (EF) <50%, or LV apical aneurysm (Class 2a).1 An ICD may be considered if there is extensive fibrosis ≥15% of LV mass detected by late gadolinium enhancement (LGE) in cardiac MRI, or if there is significant non-sustained ventricular tachycardia (NSVT) seen on an ambulatory monitor (Class 2b).1
These primary prevention recommendations differ from the older guidelines published by the European Society of Cardiology in 2014, which used the HCM Risk-SCD, the first validated risk prediction model to estimate the risk of SCD at 5 years in patients with HCM.2,3 The following criteria were used:2,3
Age
Maximum LV wall thickness (≥30 millimeter)
Left atrial size
LVOT gradient
Family history of SCD
NSVT
Unexplained syncope
Upon calculation with the above factors, the risk of SCD in 5 years is presented in a percentage that correlates with low, intermediate, and high risk. In patients with a low risk of <4%, an ICD is generally not indicated, whereas in patients with an intermediate risk of 4-6%, an ICD may be considered, and in patients with a high risk ≥6%, an ICD should be considered.2 It is important to note that this model should not be used in pediatric patients younger than 16 years old, elite athletes, or individuals with metabolic disorders.2,3
The new ACC/AHA guidelines expand upon previously published recommendations on SCD risk in HCM. These include considering newly identified markers such as ejection fraction, LV apical aneurysm, and myocardial fibrosis, which can be evaluated by cardiac MRI.1 These new recommendations help clinicians evaluate a patient's individualized risk factors and aid in shared decision conversations regarding primary prevention ICD placement in HCM.
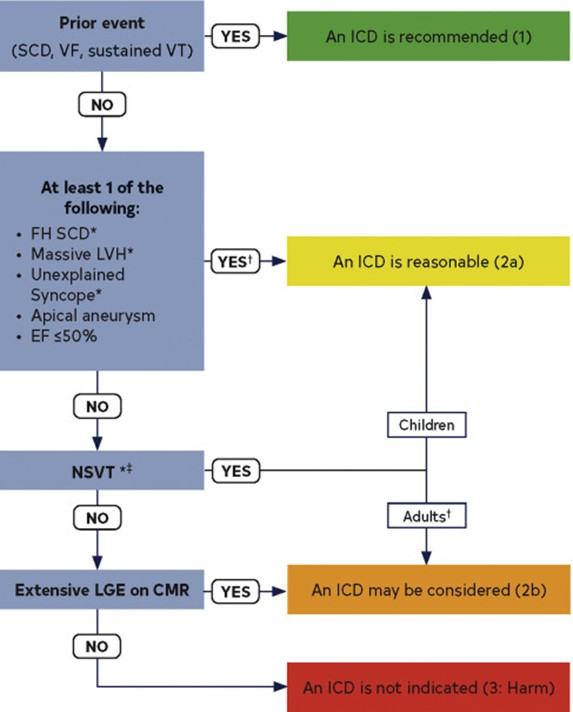
Figure 3
Figure 3
Figure 3: ICD patient selection. Ommen SR, Mital S, Burke MA, al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2020;76:3022-55.
Figure 3: ICD patient selection. Ommen SR, Mital S, Burke MA, al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2020;76:3022-55.
References
Ommen SR, Mital S, Burke MA, et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2020;76:3022-55.
Elliott PM, Anastasakis A, Borger MA, et al. 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy: the task force for the diagnosis and management of hypertrophic cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J 2014;35:2733-79.
O'Mahony C, Jichi F, Pavlou M, et al. A novel clinical risk prediction model for sudden cardiac death in hypertrophic cardiomyopathy (HCM risk-SCD). Eur Heart J 2014;35:2010-20.