A 68-year-old endurance cyclist presented after an ascending aortic aneurysm was identified incidentally on a non-contrast lung cancer screening computed tomography (CT). The ascending aorta measured 4.8 cm. He noted no exertional chest pain or change in fitness. He previously participated in cycling races but more recently had been riding with friends at a moderate pace. He was cycling 150-200 miles/week, over 5-6 rides. He was also walking and doing strength training. Past medical history was notable for hypertension (managed with valsartan and hydrochlorothiazide) and dyslipidemia. Family history was notable for an ascending aortic aneurysm in his older sister.
The patient measured 1.85m in height and 100.2kg in weight with a body mass index (BMI) of 29.2kg/m2 and a body surface area of 2.27m2. Blood pressure was 134/83mmHg. Physical exam was unremarkable without joint laxity, chest, or spinal deformity, facial, oral, or ocular abnormalities. His cardiovascular exam was normal with no murmurs.
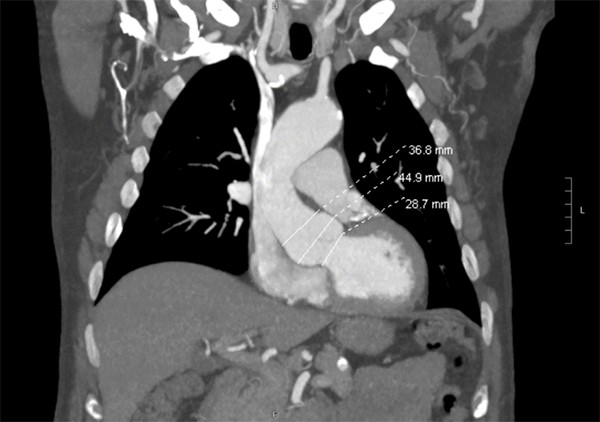
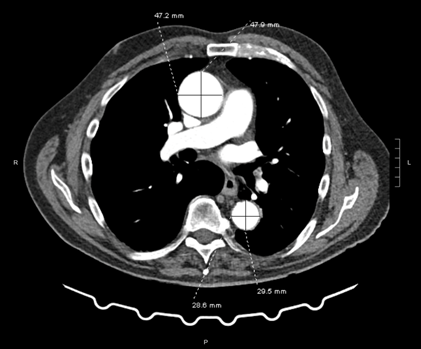
A CT angiogram (CTA) of the chest, abdomen and pelvis was performed. The aorta at sinuses of Valsalva was 4.5 cm, the ascending aorta was 4.8 cm, and a small abdominal aortic aneurysm measured 3.2 cm (Figure 1). By transthoracic echo, his aortic root was 4.5 cm (Z-score 2.63); the aortic valve was trileaflet with mild aortic insufficiency and no stenosis. Left ventricular size, thickness, and function were normal.
Figure 1A: Aortic Root Dilatation
Figure 1A
Figure 1B: Upper Ascending and Descending Aortic Dilatation
Figure 1B
Which ONE of the following is true?
Show Answer
The correct answer is: D. Pending genetic testing, the patient should undergo transthoracic echocardiogram, CTA, or magnetic resonance angiography (MRA) every 6-12 months depending on absolute aortic size and stability, Z-score, and sport intensity, with potential disqualification from competition if the aorta enlarges.
Among young athletes it is uncommon (<2%) for the aorta to exceed 34 mm in a female or 40 mm in a male. In contrast, aortic dilatation is more common among aging endurance athletes. For example, among 442 endurance athletes with a mean age of 61 years, aortic dilatation (defined by a diameter at sinuses of Valsalva or ascending aorta of ≥40 mm) was found in 21%.1 However, this patient's aorta is beyond what is commonly observed in a masters athlete and requires a workup for underlying causes, including genetic evaluation. When a dilated thoracic aorta is identified in an athlete, risk stratification with advanced imaging of the aorta with CTA or MRA and exercise testing with blood pressure assessment is recommended.2
Although the 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease does not differentiate the two entities, the aortic root should be considered separate from the upper ascending aorta.3 This distinction is important because evidence suggests aortic root dilatation is more malignant than a similar degree of dilatation of the upper ascending aorta4 and because guidelines recommend using aortic root Z-scores that incorporate height, weight, age, and sex to determine normal aortic diameter as opposed to a single dimension.5 Online tools can be used to calculate the Z-score = (observed aortic root size – expected aortic root size)/0.261.5 Aortic dilatation is confirmed when Z-score is >2.0, which corresponds to approximately 98th percentile of the general population. A Z-score of 3.0 corresponds to the 99.9th percentile.6 Mild, moderate, and severe aortic dilatation may be defined by Z-scores of 2-3, 3.01-4.0, and >4.0, respectively.
Athletes with a dilated aorta should be referred to a cardiovascular specialist and geneticist to exclude underlying disorders such as Marfan syndrome, Loeys-Dietz syndrome, familial thoracic aortic aneurysm syndrome, or bicuspid aortic valve. An individualized management plan based on shared decision-making should be developed.7,8 Such a plan should ensure abstinence from tobacco, strict blood pressure control with a target systolic blood pressure of 105-120 mmHg with beta-blockers and/or losartan, consideration of a statin (which may provide benefit through inhibition of matrix metalloproteinases9) and avoidance of fluoroquinolones given the associated risk of dissection.10 Exercise recommendations/restrictions, using a shared decision framework should be provided, along with an imaging surveillance plan to assess for progression with appropriate cessation of exercise and referral for surgical evaluation as needed. Consensus guidelines recommend avoidance of strenuous exercise and any weightlifting that requires "bearing down" or Valsalva, specifically for those with a genetic aortopathy, including bicuspid aortic valve with a Z-score >3.5, aortic root diameter >42mm, or an enlarging aorta (>0.5cm/year). Surgical referral should occur as the aortic diameter approaches an indication for surgical repair: >5.5cm in diameter, enlarging >0.5cm/year, ≥4.2cm in Loeys-Dietz syndrome, or ratio of maximal ascending or aortic root area divided by the patient's height in meters exceeding 10 in those with Marfan syndrome.3
Given the paucity of data examining the long-term outcomes of athletes with unexplained aortic dilatation and the true risk of dissection with sports participation in many genetic aortopathies such as bicuspid aortic valve, it is critical to emphasize that current exercise guidance and the recommendations above are solely expert opinion. Thus, decisions should be individualized in conjunction with experts in sports cardiology and aortopathy using shared decision-making.7 Discussion with the athlete, parents (when appropriate), and coaches/trainers should include transparency regarding potential risks and uncertainties of training and competition. The risk of aortic dissection is related to many factors, foremost of which is the severity of aortic dilation. Long-distance cycling primarily results in dynamic physiologic strain and may be more suitable than static exercise such as weightlifting in those with aortopathy. Since our patient was already cycling at a non-competitive level at this point in his athletic career, we advised that he could continue moderate-intensity cycling. He was encouraged to limit isometric activities (such as sit-ups, push-ups, and pull-ups), and to avoid lifting weights he could not repeat 10 times without difficulty. Imaging at 6 months showed no change in aortic diameter.
References
Churchill TW, Groezinger E, Kim JH, et al. Association of ascending aortic dilatation and long-term endurance exercise among older masters-level athletes. JAMA Cardiol 2020;5:522-31.
Pelliccia A, Sharma S, Gati S, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J 2021;42:17-96.
Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. J Am Coll Cardiol 2010;55:1509-44.
Kalogerakos PD, Zafar MA, Li Y, et al. Root dilatation is more malignant than ascending aortic dilation. J Am Heart Assoc 2021;10:e020645.
Maron BJ, Zipes DP, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: preamble, principles, and general considerations: a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015;66:2343-49.
Devereux RB, de Simone G, Arnett DK, et al. Normal limits in relation to age, body size and gender of two-dimensional echocardiographic aortic root dimensions in persons ≥15 years of age. Am J Cardiol 2012;110:1189-94.
Martinez MW, Kim JH, Shah AB, et al. Exercise-induced cardiovascular adaptations and approach to exercise and cardiovascular disease: JACC State-of-the-Art Review. J Am Coll Cardiol 2021;78:1453-70.
Salameh MJ, Black JH 3rd, Ratchford EV. Thoracic aortic aneurysm. Vasc Med 2018;23:573-78.
Stein LH, Berger J, Tranquilli M, Elefteraides JA. Effect of statin drugs on thoracic aortic aneurysms. Am J Cardiol 2013;112:1240-45.
Pasternak B, Inghammar M, Svanström H. Fluoroquinolone use and risk of aortic aneurysm and dissection: nationwide cohort study. BMJ 2018;360:k678.