A 65-year-old female with stage 1 invasive ductal carcinoma breast cancer, treated with lumpectomy in September 2021 with adjuvant anastrozole chemotherapy and radiation therapy starting in November 2021, presented with pleuritic chest pain. Her pain first started in January 2022 after receiving 16 sessions of radiation treatment and she had multiple emergency department visits for recurrent chest pains. The pain was sharp in nature, located primarily in the left chest, radiated to the left arm, and was exacerbated by movement and change in position. She experienced a significant decrease in her activity level because of the pain. She also endorsed palpitations and shortness of breath but denied orthopnea, paroxysmal nocturnal dyspnea (PND), dizziness, syncope, and leg swelling. Previous workup included persistently elevated inflammatory markers and a computed tomography (CT) scan of the chest which showed post-radiation fibrosis and scarring in the left upper and lower lobes, minimal scarring in the right lobe, a left pleural effusion, and a new moderate, circumferential pericardial effusion. Patient had been taking prednisone 10 mg daily and colchicine 0.6 mg twice daily without resolution of her symptoms. Physical exam showed a normotensive patient with regular rate and rhythm, no friction rub or pericardial knock, no murmurs, and no jugular vein distention (JVD). Patient did not have peripheral edema and had grade 2/4 distal pulses bilaterally.
Past Medical History
Other medical history was pertinent for hypertension, hyperlipidemia, coronary artery calcifications and paroxysmal atrial fibrillation. She denied any history of cardiac surgeries, autoimmune conditions, tuberculosis, or recent viral infections.
Investigations
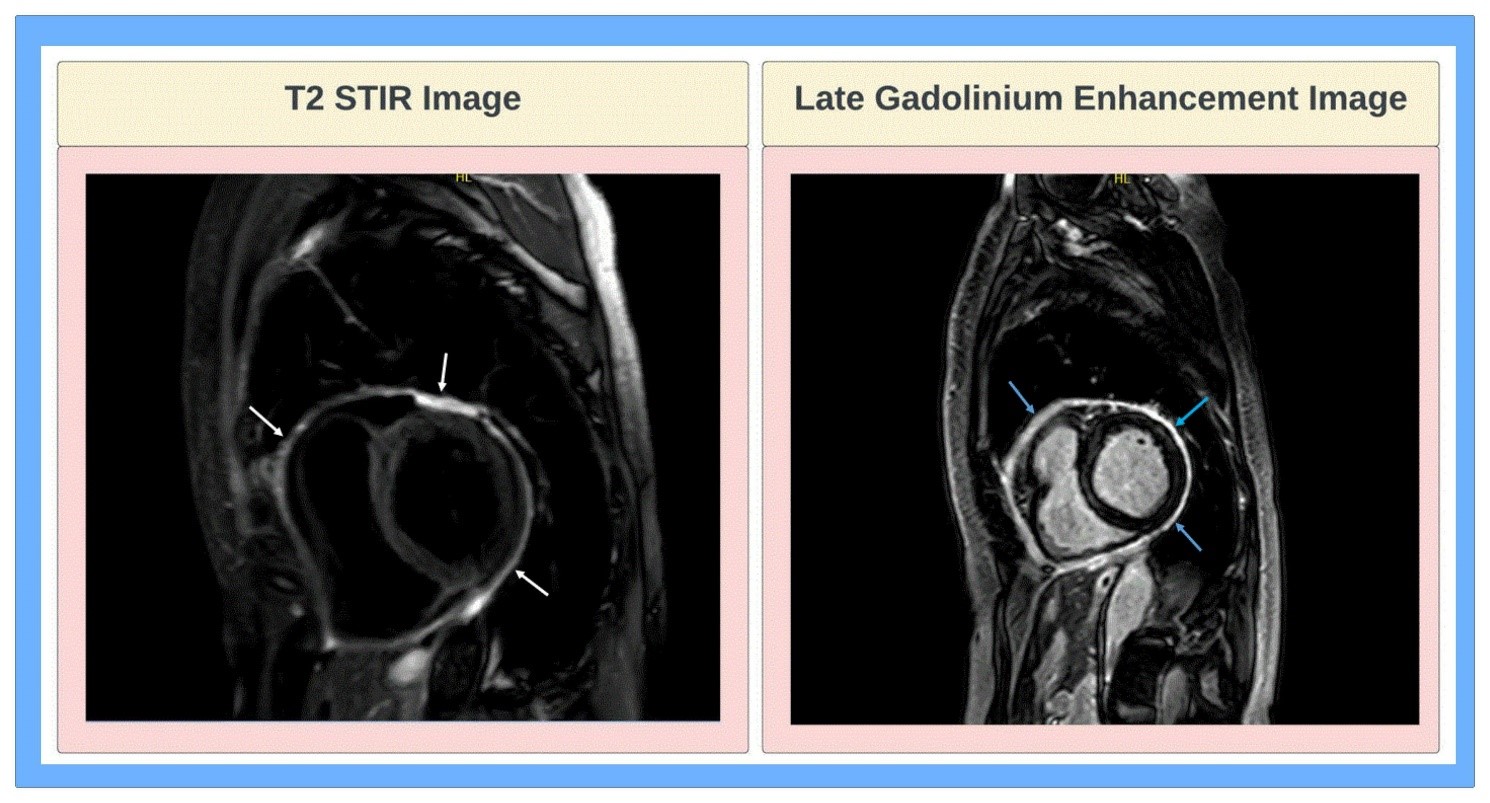
Laboratory studies were pertinent for negative Westergren sedimentation rate of 13 mm/hr, negative C-reactive protein of <0.3 mg/dL, elevated N-terminal prohormone brain natriuretic peptide (NTproBNP) of 1,138 pg/mL, and slightly elevated high sensitivity troponin T of 22 ng/L. Electrocardiogram showed sinus rhythm at a rate of 60 beats per minute, normal axis, normal intervals, and non-specific T-wave inversions in the inferior leads. Echocardiogram showed no evidence of pericardial effusion or constrictive physiology, normal left ventricular systolic and diastolic function with ejection fraction of 65%, normal right ventricular systolic function, and no significant valvular abnormalities. Cardiac magnetic resonance imaging (CMR) showed mildly increased pericardial thickness measuring 4 mm without pericardial effusion, moderate pericardial late gadolinium enhancement (LGE) and mild pericardial edema on T2 weighted, no evidence of constrictive physiology, normal biventricular size, and systolic function with no myocardial delayed enhancement to indicate prior ischemic damage or interstitial fibrosis (Figure 1). Patient was thus diagnosed with pericarditis, likely radiation induced.
What is the best next step for this patient's chest pain?
Show Answer
The correct answer is: A. Commence on non-steroidal anti-inflammatory drugs (NSAIDs) and continue colchicine and steroids.
Radiation therapy has gained increased use in the treatment of several malignancies, including breast cancer, as it has demonstrated significant survival benefit in cancer patients.1 Radiation therapy has the potential of causing inflammatory damage to nearby organs. Radiation-induced heart disease is a spectrum of cardiotoxic disorders resulting from radiation therapy and can potentially encompass damage to all cardiac structures including the pericardium, myocardium, valves, coronary arteries, and electrical conduction system.2
Radiation-induced pericardial disease consists of pericardial effusion, acute pericarditis, delayed pericarditis, and constrictive pericarditis. Acute pericarditis is rare and typically occurs during active radiation treatment; it consists of typical pericarditis signs and symptoms including chest pain, fever, friction rub, and ST segment elevations or depressions on electrocardiogram (ECG).3 Radiation-induced acute pericarditis is often self-limiting and approximately half of patients do not require intervention.3
Delayed pericarditis is similar in symptomatology to acute pericarditis but presents months to years following radiation therapy, with a median time to presentation of 12 months.3 The risk of developing radiation pericarditis is increased with higher doses and with exposure to increased areas of the heart (>30%).3 It is estimated that 20% of patients will progress to having chronic or constrictive pericarditis which is significantly higher than that seen with pericarditis of most other etiologies.4 Treatment, when indicated, consists of standard pericarditis treatment including NSAIDs and colchicine, with steroids reserved as second-line therapy for patients who fail initial treatment.4 Interleukin-1 (IL-1) inhibitors have not been well studied in the treatment of radiation-induced pericarditis, however their potential efficacy presents an interesting avenue for further research based on our understanding of IL-1 as a pathophysiologic mediator of radiation-induced heart disease.5
Asymptomatic pericardial effusion is the most common manifestation of radiation-induced pericardial disease and requires serial monitoring but does not typically require intervention.6 Treatment, when indicated, includes anti-inflammatory therapy with pericardiocentesis being performed for symptomatic or hemodynamically-compromising effusions.6 Constrictive pericarditis is the most severe form of radiation-induced pericardial disease, occurring as a result of fibrosis and thickening of the pericardium, and often requires pericardiectomy.7 However, mortality rates associated with pericardiectomy are higher in these patients, likely due to the presence of concomitant valvular, myocardial, or coronary artery disease and mediastinal fibrosis resulting from radiation therapy.8
Our patient was diagnosed with radiation-induced pleuropericarditis which was treated with multiple courses of prednisone and colchicine 0.6 mg two times a day. Her first course of prednisone was stopped abruptly after 2 weeks which resulted in recurrence of her symptoms. Treatment of radiation-induced pericarditis is the same as pericarditis of other etiologies and consists of NSAIDs and colchicine as first-line, with corticosteroids used as a second-line agent. This patient has not been treated with the appropriate regimen, so the correct answer is to start her on NSAIDs and continue colchicine and steroids, with a plan for a steroid taper once her symptoms resolve and her inflammatory markers normalize.
References
Belzile-Dugas E., Eisenberg MJ. Radiation-induced cardiovascular disease: review of an underrecognized pathology. J Am Heart Assoc 2021;10:e021686.
Wang H, Wei J, Zheng Q, et al. Radiation-induced heart disease: a review of classification, mechanism, and prevention. Int J Biol Sci 2019;15:2128–38.
Ghosh AK, Crake T, Manisty C, Westwood M. Pericardial disease in cancer patients. Curr Treat Options Cardiovasc Med 2018;20:60.
Taunk NK, Haffty BG, Kostis JB, Goyal S. Radiation-induced heart disease: pathologic abnormalities and putative mechanisms. Front Oncol 2015;5:39.
Yeneneh BT, Allen S, Panse P, Mookadam F, Rule W. Constrictive pericarditis 5 months after radiation therapy in a 62-year-old woman with esophageal cancer. Tex Heart Inst J 2017;44:411–5.
Marinko T. Pericardial disease after breast cancer radiotherapy. Radiol Oncol 2018;53:1–5.
Murashita T, Schaff HV, Daly RC, et al. Experience with pericardiectomy for constrictive pericarditis over eight decades. Ann Thorac Surg 2017;104:742–50.