A 21-year-old professional hockey player experienced a cardiac arrest shortly after warming up for a recreational basketball game. He has no medical history and no relevant family history. He has been a multisport athlete his entire life and has never experienced cardiac symptoms or exercise limitations. After a short warm-up, he walked toward the bench, collapsed, and became unresponsive. Cardiopulmonary resuscitation was started immediately, and his initial rhythm was ventricular tachycardia. He received two defibrillations with return of spontaneous circulation in 8 minutes.
Upon arrival at the hospital, he is awake, alert, and able to follow commands. His vital signs show normotension and tachycardia. Laboratory investigations are notable for an elevated troponin-I level of 1.1 ng/mL (reference range: <0.03 ng/mL).
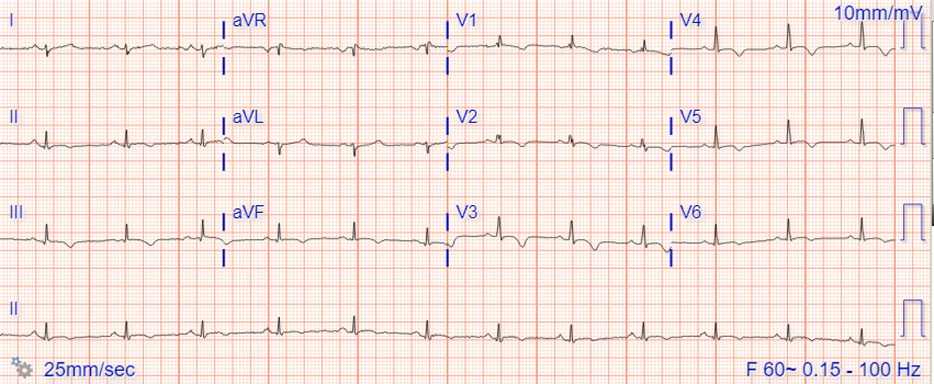
An initial electrocardiogram demonstrates sinus rhythm at a rate of 75 bpm with inferior and anteroapical T-wave inversions (Figure 1).
Figure 1
Figure 1
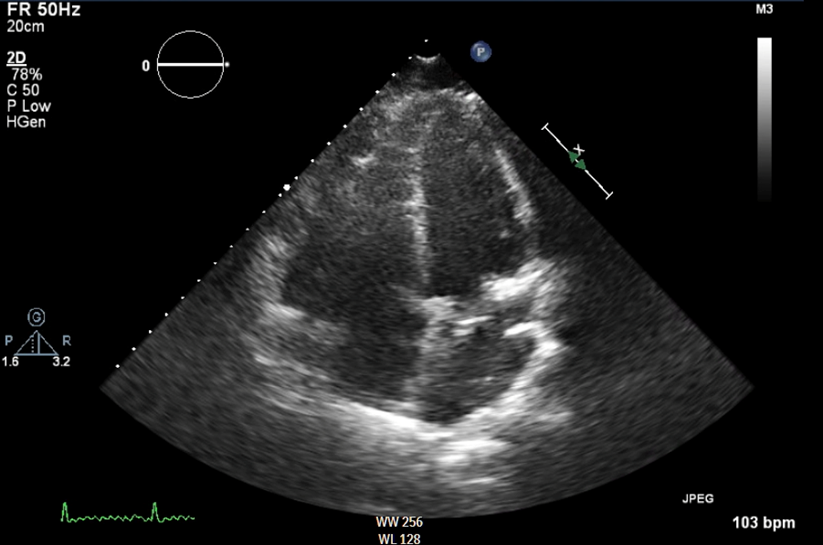
Echocardiography shows a dilated right ventricle (RV) with dyskinesia of the RV apex (Figure 2; Video 1).
Figure 2
Figure 2
Video 1
Video 1
Similarly, cardiac magnetic resonance imaging (CMR) reveals a dilated RV with reduced ejection fraction 32%, dyskinesia of the free wall and RV apex, and an RV apical thrombus (Video 2). The RV end-diastolic volume indexed to his body surface area is 110 mL/m2 (reference range: <88 mL/m2).
Video 2
Video 2
He undergoes genetic testing, which reveals positive findings for deleterious desmosomal mutation in plakophilin 2 (PKP2; Gin378Ter), which is highly specific for arrhythmogenic right ventricular cardiomyopathy (ARVC). He has a full recovery and is discharged after 5 days in the hospital.
Prior to discharge, he asks to discuss his options for returning to playing hockey. He states that hockey is his life and source of income, and he would like to continue to play at the professional level.
Which one of the following should be recommended regarding his return to play?
Show Answer
The correct answer is: C. Implantable cardiac defibrillator and beta-blocker with recommendation to not return to professional hockey.
This athlete was diagnosed with ARVC, a genetic cardiomyopathy with a prevalence of between 1:1,000 and 1:5,000.1 ARVC is a common cause of sudden cardiac death (SCD) in athletes that has been shown to be present in 2-36% of athletic persons who die of SCD.2 ARVC is characterized by replacement of RV myocardial tissue with fibrofatty tissue,3 leading to ventricular arrhythmias (VAs), sudden death, and, less frequently, ventricular failure. ARVC falls under the umbrella of arrhythmogenic cardiomyopathy (ACM), which is a more comprehensive designation that also includes biventricular and dominant–left ventricular phenotypic variants. Up to two-thirds of patients with ARVC have mutations in genes encoding proteins in the intercalated disc, most commonly desmosomal proteins, but a positive genetic mutation is not required for diagnosis.4,5 Updated criteria for assessment of ACM have been proposed in the 2020 international criteria for ACM (Table 1), which include revised criteria to the 2010 Task Force Criteria for right-sided ACM and for the first time include criteria for left-sided ACM.5
Table 1
Global or regional dysfunction and structural alteration
Major 2DE, CMR, or angiography:
Regional RV akinesia, dyskinesia, or bulging
plus:
Global RV dilatation (increase of RVEDV); or
Global RV systolic dysfunction (reduction of RVEF)
Minor By 2DE, CMR, or angiography:
Regional RV akinesia, dyskinesia, or aneurysm of RV free wall
Tissue characterization
Major By CMR:
Transmural LGE of ≥1 RV region(s) (inlet, outlet, and apex)
Major By EMB (limited indications):
Fibrous replacement of the myocardium in ≥1 sample, with or without fatty tissue
Repolarization abnormalities
Major
Inverted T waves in the right precordial leads (V1, V2, and V3) or beyond in individuals with complete pubertal development (in the absence of complete RBBB)
Minor
Inverted T waves in leads V1 and V2 in individuals with completed pubertal development (in the absence of complete RBBB)
Inverted T waves in leads V1 to V4 in individuals with completed pubertal development in the presence of complete RBBB
Depolarization and conduction abnormalities
Minor
Epsilon wave (reproducible low‐amplitude signals between the end of the QRS complex to the onset of the T wave) in the right precordial leads ( V1 to V3)
Terminal activation duration of QRS ≥55 msec measured from the nadir of the S wave to the end of the QRS, including R′, in leads V1 to V3 (in the absence of complete RBBB)
Arrhythmias
Major
Frequent ventricular extrasystoles (>500/24 h), nonsustained or sustained VT of LBBB morphology
Minor
Frequent ventricular extrasystoles (>500/24 h), NSVT or sustained VT of LBBB morphology with inferior axis ("RVOT pattern")
Family history/genetics
Major
ACM confirmed in a first‐degree relative who meets diagnostic criteria
ACM confirmed pathologically at autopsy or surgery in a first‐degree relative
Identification of a P/LP ACM mutation in the patient under evaluation
Minor
History of ACM in a first‐degree relative in whom it is not possible or practical to determine whether the family member meets diagnostic criteria
Premature sudden death (<35 y of age) due to suspected ACM in a first‐degree relative
ACM confirmed pathologically or by diagnostic criteria in a second‐degree relative
Possible ARVC equals two minor criteria. Borderline ARVC equals one major plus two minor or three minor criteria. Definite ARVC equals two major or one major plus two minor or four minor criteria.2DE = two-dimensional echocardiography; ACM = arrhythmogenic cardiomyopathy; CMR = cardiac magnetic resonance; EMB = endomyocardial biopsy; LBBB = left bundle branch block; LGE = late gadolinium enhancement; NSVT = nonsustained ventricular tachycardia; P/LP = pathogenic or likely pathogenic; RBBB = right bundle branch block; RV = right ventricular; RVEDV = right ventricular end-diastolic volume; RVEF = right ventricular ejection fraction; RVOT = right ventricular outflow tract; VT = ventricular tachycardia.Modified with permission from Corrado D, Zorzi A, Cipriani A, et al. Evolving diagnostic criteria for arrhythmogenic cardiomyopathy. J Am Heart Assoc 2021;Sep 17:[Epub ahead of print].
In patients with ARVC, sudden death is commonly reported during exercise.3,6,7 Data show that exercise can increase penetrance and arrhythmia risk in patients who are gene carriers of ARVC.8 Animal data from plakoglobin-deficient mouse models revealed that mice that underwent intense exercise developed phenotypic ARVC with RV dilation and increased VAs.8 Similarly, in a study of endurance athletes who were desmosomal mutation carriers, symptoms developed at a younger age in athletes (30 vs. 41 years of age) than nonathletes.9 Further, 64% of endurance athletes were symptomatic at the time of diagnosis compared with 26% of nonathletes. Athletes were also more likely to have VAs (55% vs. 26%) and to develop stage C heart failure (18% vs. 0%) than nonathletes.9
Gene mutations in ARVC result in disruption of normal cell adhesion, cell-to-cell communication, and mechanical stability. Vigorous and prolonged exercise may accelerate disease progression in ARVC through repetitive bouts of increased sheer stress on the thin-walled, compliant RV. This stress is thought to promote breakdown of the abnormal proteins within the intercalated discs and leads to fibrofatty replacement of the myocytes.10-12
Studies have tried to identify an exercise threshold at which there is an increased risk of arrhythmias and/or cardiac arrest. Findings from mouse models with plakoglobin (PKP2) mutations revealed that RV dysfunction was seen with more extreme exercise than with recreational exercise.12,13 Similarly, in humans, exercise has been shown to be dose-dependently associated with risk of sustained VAs in ARVC starting at >30 metabolic equivalents of each individual activity multiplied by the duration in hours per week (METh/week) but no increased risk of VAs below 15-30 METh/week.14 Regarding patients with implantable cardiac defibrillators at higher risk, data suggest that reduction in exercise intensity and duration results in the greatest reduction in arrhythmia events.15
This patient wanted to continue to train at a professional level despite a confirmed diagnosis of ARVC, advanced phenotypic disease, and previous cardiac arrest. The 2015 American Heart Association/American College of Cardiology (AHA/ACC) Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities state that athletes with a definitive diagnosis of ARVC, as in this patient, should not participate in competitive sports except for class 1A sports (e.g., cricket, curling, golf).16 The European Society of Cardiology (ESC) Guidelines on Sports Cardiology and Exercise in Patients With Cardiovascular Disease provide a class IIa recommendation to consider 150 minutes of low-intensity exercise (equivalent to <7.5 METh/week) in individuals with ARVC (including those who are gene positive/phenotype negative) and class IIb recommendation to consider low- to moderate-intensity exercise in those without high-risk features (similar to <15 METh/week).17
This patient was placed on a beta-blocker at the time of his index hospitalization and a defibrillator was placed prior to discharge. He was counseled to forgo professional hockey. However, the physical and mental health risk of a sedentary lifestyle are not trivial for a young man and must be considered in the overall management plan. Using a shared decision-making approach, the recent data were reviewed, and it was suggested that low- to moderate-intensity exercise may be reasonable, but it was highlighted that these data are not directly applicable for him because he already experienced a cardiac arrest. A primarily low-intensity exercise regimen with avoidance of high-intensity and high-volume training was prescribed with close follow-up.
References
Peters S, Trümmel M, Meyners W. Prevalence of right ventricular dysplasia-cardiomyopathy in a non-referral hospital. Int J Cardiol 2004;97:499-501.
Harmon KG. Incidence and causes of sudden cardiac death in athletes. Clin Sports Med 2022;41:369-88.
Thiene G, Nava A, Corrado D, Rossi L, Pennelli N. Right ventricular cardiomyopathy and sudden death in young people. N Engl J Med 1988;318:129-33.
Towbin JA, McKenna WJ, Abrams DJ, et al. 2019 HRS expert consensus statement on evaluation, risk stratification, and management of arrhythmogenic cardiomyopathy. Heart Rhythm 2019;16:e301-e372.
Corrado D, Zorzi A, Cipriani A, et al. Evolving diagnostic criteria for arrhythmogenic cardiomyopathy. J Am Heart Assoc 2021;Sep 17:[Epub ahead of print].
Corrado D, Thiene G, Nava A, Rossi L, Pennelli N. Sudden death in young competitive athletes: clinicopathologic correlations in 22 cases. Am J Med 1990;89:588-96.
Basso C, Corrado D, Marcus FI, Nava A, Thiene G. Arrhythmogenic right ventricular cardiomyopathy. Lancet Lond Engl 2009;373:1289-300.
Kirchhof P, Fabritz L, Zwiener M, et al. Age- and training-dependent development of arrhythmogenic right ventricular cardiomyopathy in heterozygous plakoglobin-deficient mice. Circulation 2006;114:1799-806.
James CA, Bhonsale A, Tichnell C, et al. Exercise increases age-related penetrance and arrhythmic risk in arrhythmogenic right ventricular dysplasia/cardiomyopathy-associated desmosomal mutation carriers. J Am Coll Cardiol 2013;62:1290-7.
La Gerche A, Heidbüchel H, Burns AT, et al. Disproportionate exercise load and remodeling of the athlete's right ventricle. Med Sci Sports Exerc 2011;43:974-81.
Prior D, La Gerche A. Exercise and arrhythmogenic right ventricular cardiomyopathy. Heart Lung Circ 2020;29:547-55.
Cruz FM, Sanz-Rosa D, Roche-Molina M, et al. Exercise triggers ARVC phenotype in mice expressing a disease-causing mutated version of human plakophilin-2. J Am Coll Cardiol 2015;65:1438-50.
Bosman LP, Wang W, Lie ØH, et al. Integrating exercise into personalized ventricular arrhythmia risk prediction in arrhythmogenic right ventricular cardiomyopathy. Circ Arrhythm Electrophysiol 2022;Jan 28:[Epub ahead of print].
Wang W, Orgeron G, Tichnell C, et al. Impact of exercise restriction on arrhythmic risk among patients with arrhythmogenic right ventricular cardiomyopathy. J Am Heart Assoc 2018;Jun 15:[Epub ahead of print].
Maron BJ, Zipes DP, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: preamble, principles, and general considerations: a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015;66:2343-49.
Pelliccia A, Sharma S, Gati S; ESC Scientific Document Group, et al. 2020 ESC guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J 2021;42:17-96.