A 16-year-old boy with a history of prematurity, developmental delay, and small bowel transplant at 5 years of age secondary to an intestinal volvulus presents with acute-onset left-sided body weakness progressing to right-sided weakness and arrhythmia. There is a history of chronic diarrhea but otherwise he denies fever, vomiting, cough, rhinorrhea, or syncope.
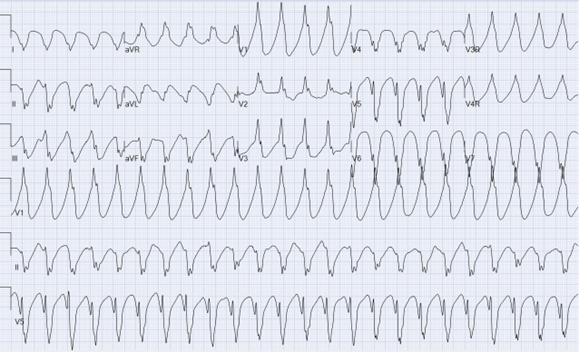
He is afebrile, tachycardic, acyanotic, and hypertensive. He is thin appearing, in no acute distress with normal mental status. He appears well hydrated and has clear breath sounds. Cardiac examination is remarkable only for tachycardia. Upper and lower extremity muscle strength is 4/5 bilaterally. A bedside echocardiogram demonstrates normal biventricular systolic function. Results of laboratory analysis reveals a mildly elevated troponin I level. An electrocardiogram (ECG) is obtained (Figure 1).
Figure 1
Figure 1
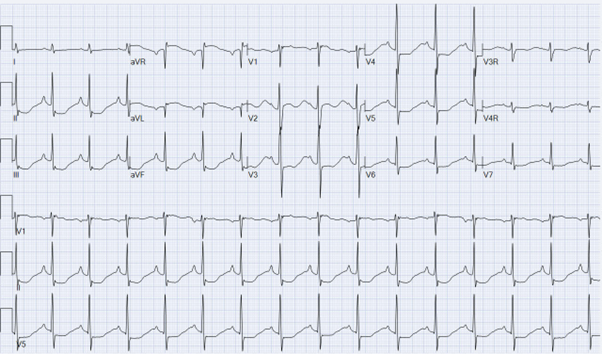
Lidocaine is administered and he is transferred to the pediatric intensive care unit for further management. The tachycardia resolves 1 hour after presentation. A subsequent ECG and telemetry tracings after resolution of the tachycardia are recorded (Figures 2, 3, 4):
Figure 2
Figure 2
Figure 3
Figure 3
Figure 4
Figure 4
Which one of the following is the most likely cause of his presentation?
Show Answer
The correct answer is: D. Hypokalemia.
The combination of stable monomorphic ventricular tachycardia (VT) (Figure 1), frequent ectopy and ST changes (Figures 2, 3, 4) are most consistent with severe hypokalemia. Hypokalemia is a common electrolyte abnormality caused by poor potassium intake, gastrointestinal tract (GI) or urinary tract losses, and shifts in extracellular concentrations. In uncomplicated hypokalemia, ECG changes include ST-segment depression, a decrease in T-wave amplitude, prominent U waves, and a U-wave-to-T-wave ratio >1. Severe hypokalemia, however, is known to cause potentially fatal cardiac arrhythmias including torsades de pointes, monomorphic VT (as in this patient), and, in rare cases, bidirectional VT.1,2 Additionally, ECG changes with hypokalemia have been reported to mimic ST elevation in adults.3 In this case, laboratory results sent in the emergency department upon presentation revealed potassium level 1.8 mmol/L (hemolyzed sample). A history of chronic diarrhea, weakness, stable VT, and ST changes should lead to a high index of suspicion for hypokalemia.
Brugada syndrome is unlikely in this case because VT due to Brugada syndrome is typically unstable. Additionally, the ECG in sinus rhythm in these patients demonstrates incomplete right bundle branch block along with ST elevation in the anterior precordial leads (leads V1 through V3). In hypercalcemia, patients can present with weakness and ST changes. However, in these patients, the QTc shortens and bradyarrhythmias are more common.4 Myocardial infarction is a reasonable possibility in this patient. However, with only a mild troponin level elevation, lack of chest pain, normal biventricular systolic function, and age at presentation, this diagnosis is less likely. Long QT syndrome is an important consideration in the differential diagnosis; however, associated VT is typically polymorphic and ST changes would not be expected.
After resolution of the VT (Figure 1), he develops frequent ectopy (Figure 2) that resolves with potassium levels consistently >3 mmol/L. Once his potassium level normalizes, his ST changes (Figures 2, 3, 4) resolve. Nephrology is consulted on admission and determines that urine electrolyte levels are not consistent with renal wasting. Therefore, the hypokalemia was thought to be secondary to GI losses in combination with inadequate intake. Once his potassium level stabilizes, he is started on oral potassium supplementation and has no further sustained ventricular arrhythmias while hospitalized. He is seen in follow-up with stable potassium levels on continued supplementation and no recurrence of symptoms. The exact etiology of his hypokalemia is never definitively proven.
Hypokalemia is a medical emergency and must be promptly recognized.
References
Xie Y, Han J, Liu J, Hao J, Zu X, Hao Y. A case of hypokalemia-induced bidirectional ventricular tachycardia. J Int Med Res 2020;48:[Epub ahead of print].
Rodriguez AP, Badiye A, Lambrakos LK, Ghodsizad A, Myerburg RJ, Goldberger JJ. Refractory ventricular tachycardia storm associated with severe hypokalemia in Fanconi syndrome. HeartRhythm Case Rep 2019;5:374-8.
Chua CE, Choi E, Khoo EYH. ECG changes of severe hypokalemia. QJM 2018;111:581-2.
Durant E, Singh A. ST elevation due to hypercalcemia. Am J Emerg Med 2017;35:[Epub ahead of print].