The patient is a 62-year-old woman with a history of paroxysmal atrial fibrillation (AF), sinus node dysfunction (SND), and ventricular tachycardia status/post dual-chamber implantable cardioverter-defibrillator. Her medication list includes metoprolol, lisinopril, potassium chloride, magnesium, and dofetilide. She is seen at the antiarrhythmic clinic for her routine scheduled visit. She has been doing fairly well, with rare, skipped beats. She denies near-syncope, syncope, lightheadedness, dizziness, and shortness of breath.
Her laboratory data show serum potassium level 4.4 mmol/L, serum magnesium level 2.2 mg/dL, creatinine level 1.01 mg/dL, and glomerular filtration rate 63 mL/min/1.73 m2.
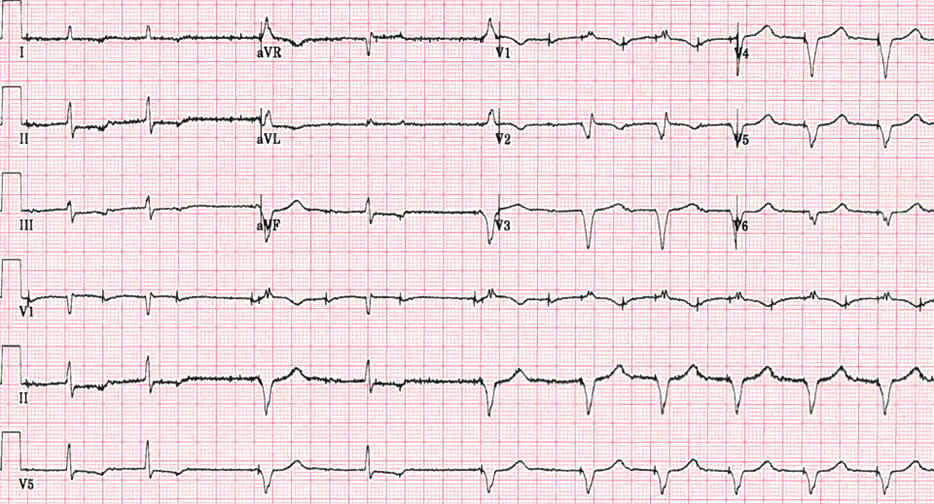
An electrocardiogram (ECG) is performed (Figure 1).
Figure 1
Figure 1
Which one of the following is the most likely explanation for this ECG?
Show Answer
The correct answer is: D. Normal pacemaker programming mode.
The ECG shows an atrial paced rhythm with heart rate 75 bpm. The first, second, and fifth beats conduct via the intrinsic AV conduction resulting in a narrow QRS complex. The third and sixth beats exhibit loss of AV conduction followed with AV sequential paced beats with short AV delay 80 msec followed with sequential paced rhythm with AV delay 340 msec.
The ECG findings are related to managed ventricular pacing (MVP), an algorithm that is intended to minimize unnecessary right ventricular pacing (RVP) by enhancing intrinsic AV conduction. MVP is an algorithm that is based on atrial-based pacing (AAIR or AAI mode) as the primary pacing mode with backup ventricular pacing if AV conduction is lost, which results in switching from AAIR or AAI mode to DDDR or DDD mode with short AV delay 80 msec followed with cyclic AV conduction evaluation. The first AV conduction evaluation occurs after 1 min followed with progressively longer intervals (2, 4, 8, 16 min. . .) up to 16 hours, then occurs every 16 hours. If the intrinsic AV conduction has recovered, then the device will switch back to AAIR or AAI mode.
If two of four recent beats are without native QRS complex (two of four P waves without AV conduction), then the device identifies persistent loss of AV conduction resulting in pacemaker switches from AAIR or AAI to the dual-chamber mode (DDDR or DDD) with the programmed AV interval. The algorithm uses 80 msec as the pacing interval on the first beat after the nonconducted beat.
It is well established that ventricular pacing results in interventricular dyssynchrony. Sweeney et al. reported that ventricular pacing increases the incidence of AF and heart failure (HF) hospitalization in patients with SND and normal baseline QRS duration.1
Udo et al. reported a steady increase of 8% risk of HF death for each 10% increase in RVP.2
Neilson et al. reported that an atrial-based pacing mode (AAIR) compared with DDDR in patients with SND results in a lower incidence of AF, left atrial enlargement, and left ventricular enlargement.3
An MVP algorithm (AAIR<=>DDDR) should be used in patients with SND and normal AV conduction to enhance intrinsic AV conduction and minimize ventricular pacing.
There is no ventricular undersensing because there is no paced ventricular beats in the third and sixth beats. Thus, answer choice A is an incorrect choice.
There is no loss of ventricular capture in the third and sixth beats because there are no pacing spikes between the third and fourth beats, or between the sixth and seventh atrial paced beats. Thus, answer choice B is an incorrect choice.
There is no AV Wenckebach because the first and second paced atrial beats have the same AV delay at 440 msec. Thus, answer choice C is an incorrect choice.
References
Sweeney MO, Hellkamp AS, Ellenbogen KA, et al. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation 2003;107:2932-7.
Udo EO, van Hemel NM, Zuithoff NP, Doevendans PA, Moons KG. Risk of heart failure- and cardiac death gradually increases with more right ventricular pacing. Int J Cardiol 2015;185:95-100.
Nielsen JC, Kristensen L, Andersen HR, Mortensen PT, Pedersen OL, Pedersen AK. A randomized comparison of atrial and dual-chamber pacing in 177 consecutive patients with sick sinus syndrome: echocardiographic and clinical outcome. J Am Coll Cardiol 2003;42:614-23.