The patient is a 62-year-old man with a history of hypertension, coronary artery disease status/post stent placement, HIV, chronic obstructive pulmonary disease, and squamous cell carcinoma status/post chemoradiation and tracheostomy who presents for planned admission to undergo repair of persistent tracheostomy. A postprocedure cardiac monitor shows wide QRS rhythm with alternating narrow QRS. He denies any chest pain, palpitation, dizziness, lightheadedness, near-syncope, or syncope.
An electrocardiogram (ECG) is performed (Figure 1).
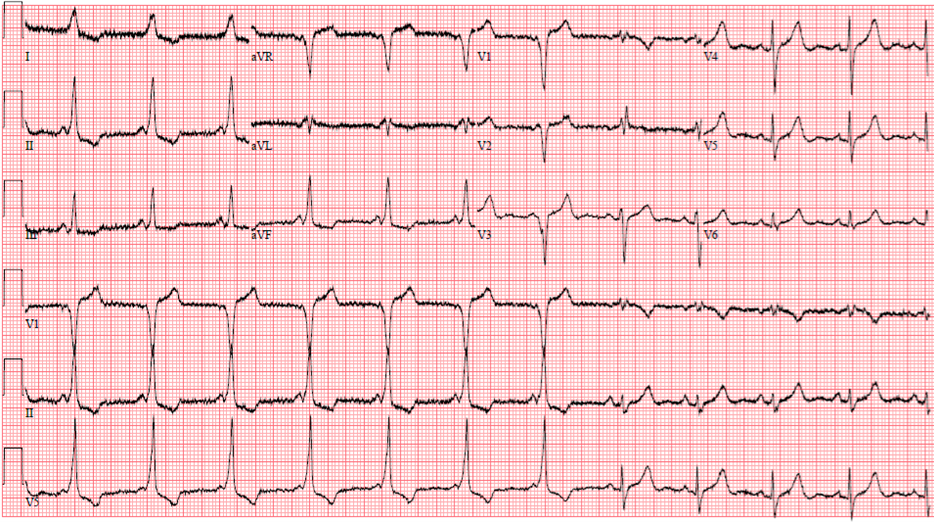
Figure 1
Figure 1
Which one of the following is the most appropriate next step?
Show Answer
The correct answer is: C. Clinical follow-up.
The ECG demonstrates sinus rhythm with heart rate 69 bpm. The beginning of the ECG starts with manifest pre-excitation with a short P-R interval of 100 msec and a wide QRS complex of 125 msec with slurring of the upstroke of the QRS complex (delta wave: fusion between anterograde conduction of the accessory pathway and the atrioventricular node His-Purkinje system).
The ECG changed from manifest pre-excitation to sinus rhythm with unremarkable P-R interval of 180 msec and unremarkable QRS duration of 100 msec with loss of the delta wave. Therefore, this patient has intermittent pre-excitation.
During evaluation of patients with manifest pre-excitation, there is a concern for sudden cardiac death, especially in those with symptomatic tachycardia, multiple accessory pathways, and pre-excited atrial fibrillation (AF) with R-R interval <250 msec.1
Intermittent pre-excitation suggests a benign prognosis if patients develop AF. This finding was reported in 1983 by Klein et al.; namely, that intermittent pre-excitation suggests a longer anterograde effective refractory period of the accessory pathway and, as such, is a predictor of poor anterograde conduction over the accessory pathway compared with persistent pre-excitation (380 msec).2
However, case reports have shown that patients with intermittent pre-excitation presenting with symptoms of palpitations, near-syncope, or syncope require an electrophysiology study (EPS) and consideration of ablation of the accessory pathway.3,4 Pietersen et al. document a rare case of a 71-year-old woman with stable ischemic heart disease and implanted pacemaker who experienced several episodes of syncope and several documented episodes of ventricular fibrillation; her ECG showed intermittent pre-excitation.5
The present patient was asymptomatic with intermittent pre-excitation; therefore, there is no need for medical or invasive intervention (answer choices A and B are incorrect choices).
He does not have symptomatic sinus node dysfunction, heart block, tachycardia-bradycardia syndrome, or pause; therefore, he does not need a pacemaker (answer choice D is an incorrect choice).
The correct answer choice is clinical follow-up. If he develops symptoms of tachycardia, including palpitations, dizziness, lightheadedness, syncope, documented supraventricular tachycardia, or AF, then he will benefit from an EPS and ablation.
References
Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2016;67:e27-e115.
Klein GJ, Gulamhusein SS. Intermittent preexcitation in the Wolff-Parkinson-White syndrome. Am J Cardiol 1983;52:292-6.
Larson NP, Rosenthal JB, Bridwell RE, Tannenbaum L, Cibrario A. Hide and seek: intermittent preexcitation Wolff-Parkinson-White syndrome case report and management overview. Cureus 2020;12:[ePub ahead of print].
Jastrzębski M, Kukla P, Pitak M, Rudziński A, Baranchuk A, Czarnecka D. Intermittent preexcitation indicates "a low-risk" accessory pathway: time for a paradigm shift? Ann Noninvasive Electrocardiol 2017;22:[ePub ahead of print].
Pietersen AH, Andersen ED, Sandøe E. Atrial fibrillation in the Wolff-Parkinson-White syndrome. Am J Cardiol 1992;70:38A-43A.