A 78-year-old woman with a history of bicuspid aortic valve (BAV) and hyperlipidemia presents to the emergency department (ED) with generalized weakness, fatigue, unintentional weight loss, and nausea.
On examination, she is afebrile, has blood pressure 109/72 mm Hg, and has a regular heart rate of 71 bpm. There was no mention of murmur or peripheral embolic findings on initial physical examination by the ED clinician. Her laboratory values are significant for hemoglobin level 13 g/dL, white blood cell count 10 kU/L, and elevated high-sensitivity troponin level 62 ng/L.
Because of an episode of supraventricular tachycardia in the ED, a transthoracic echocardiogram (TTE) is ordered. Images from the apical five-chamber (A5C) view (Video 1) and parasternal right ventricular inflow view (Video 2) are obtained.
Video 1
Video 1
Video 2
Video 2
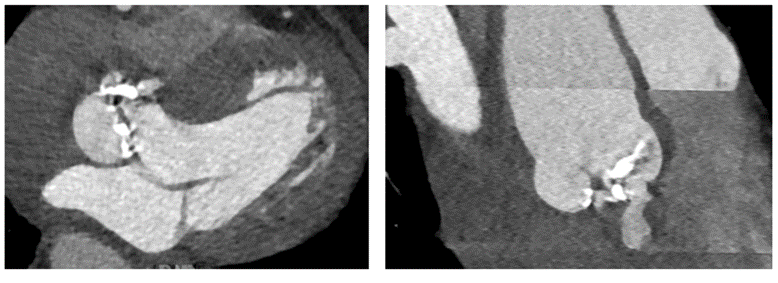
On the basis of these findings, she is admitted to the hospital and blood cultures are drawn, which grow Enterococcus faecium. A transesophageal echocardiogram (TEE) is performed. Biplane images of the aortic valve (AoV) in the midesophageal short-axis and long-axis views of the AoV (Video 3), and a transgastric basal short-axis view (Video 4), are obtained. On the basis of the need for further anatomical characterization, a contrast-enhanced cardiac computed tomography (CT) is performed (Figure 1). During her hospitalization, she has mild progressive prolongation of her P-R interval on electrocardiography but does not develop any advanced heart block or heart failure symptoms.
Video 3
Video 3
Video 4
Video 4
Figure 1
Figure 1
On the basis of the multimodal imaging findings in this case, which one of the following is the most likely diagnosis?
Show Answer
The correct answer is: E. Aortic annular abscess into the tricuspid annulus.
The best explanation for the findings is aortic annular abscess into the tricuspid annulus. Multimodality imaging was key to identifying what was eventually surgically confirmed to be an abscess extending from the aortic annulus into the septum and tricuspid annulus. The tract does not empty into a cardiac chamber; accordingly, a diagnosis of fistula cannot be made.
TTE was critical for first identifying a large mass occupying much of the tricuspid annular plane but without clear attachment to a tricuspid leaflet. The A5C view suggested continuity with the ventricular septum and medial aortic annulus. This study was also useful for confirming the presence of extensive AoV thickening and calcification, which serves as a predisposition for IE. The TEE confirmed the presence of severe thickening, calcification, and stenosis of a BAV, but without clear vegetation. However, the study also showed the presence of a cystic structure at the medial tricuspid annulus just below the level of the aortic annulus, which, when taken into context of the clinical presentation, most likely represents abscess extending inferiorly from the aortic annulus and adjacent septum into the tricuspid annulus. Studies of patients without prosthetic valves have demonstrated a much greater ability to detect abscess formation with TEE than with TTE.1
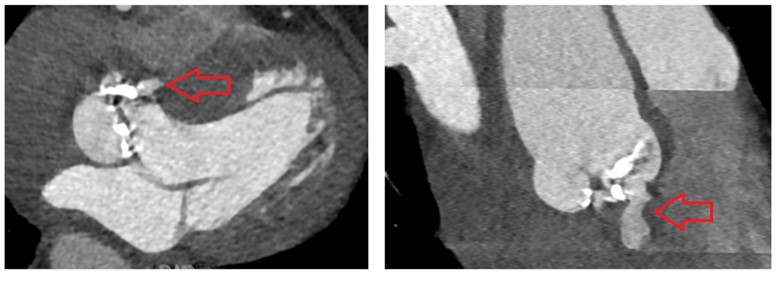
Contrast-enhanced CT imaging was vital for confirming an aortic annular abscess that was not well visualized on echocardiography (Figure 2, red arrows).2 Nonrandomized studies have reported on the complementary role of CT in diagnosing and characterizing complex abscesses in patients with IE.3 In this case, the use of multiplanar imaging assisted not only in confirming the diagnosis but also in surgical planning.
Figure 2
Figure 2
The abscess was surgically debrided and repaired using bovine pericardial repair of the abscess origin in the aortic root. Because of involvement of the aortic annulus and severely calcified valve, the patient underwent AoV replacement with a bioprosthetic valve and aortic graft. In addition, the tricuspid valve was replaced with a bioprosthesis because of tricuspid regurgitation and extensive anatomical changes of the tricuspid annulus after debridement.
This case of complicated IE serves to exemplify how multimodality imaging of cardiac structure, valve function, and blood pool is sometimes needed to fully understand anatomical involvement, anatomical relatedness, and functional complications of abscesses.
References
Daniel WG, Mügge A, Martin RP, et al. Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography. N Engl J Med 1991;324:795-800.
Hryniewiecki T, Zatorska K, Abramczuk E, et al. The usefulness of cardiac CT in the diagnosis of perivalvular complications in patients with infective endocarditis. Eur Radiol 2019;29:4368-76.
Feuchtner GM, Stolzmann P, Dichtl W, et al. Multislice computed tomography in infective endocarditis: comparison with transesophageal echocardiography and intraoperative findings. J Am Coll Cardiol 2009;53:436-44.