A 67-year-old African American woman with a history of end-stage renal disease (ESRD), hypertension, lumbar stenosis, and persistent atrial fibrillation (AF) with two ablations presents with progressive fatigue and dyspnea on exertion over the previous 6 months.
Her vital signs include blood pressure 111/68 mm Hg in the supine position, dropping to 85/62 mm Hg on standing, and an irregularly irregular rhythm at 88 bpm. Physical examination reveals a grade 2/6 systolic ejection murmur at the upper left sternal border, end-inspiratory crackles in the lower lung field, and 1+ bilateral edema. Electrocardiography shows AF with normal voltage. An echocardiogram obtained before the clinic visit is available (Videos 1, 2; Figures 1, 2). The serum free light chain (sFLC) kappa/lambda (κ/λ) ratio is 3.0 in the context of ESRD. Serum immunofixation electrophoresis (SIFE) and urine immunofixation electrophoresis (UIFE) show no monoclonal protein spike.
Video 1: Parasternal Long-Axis View
Video 1
Video 2: Apical Four-Chamber View
Video 2
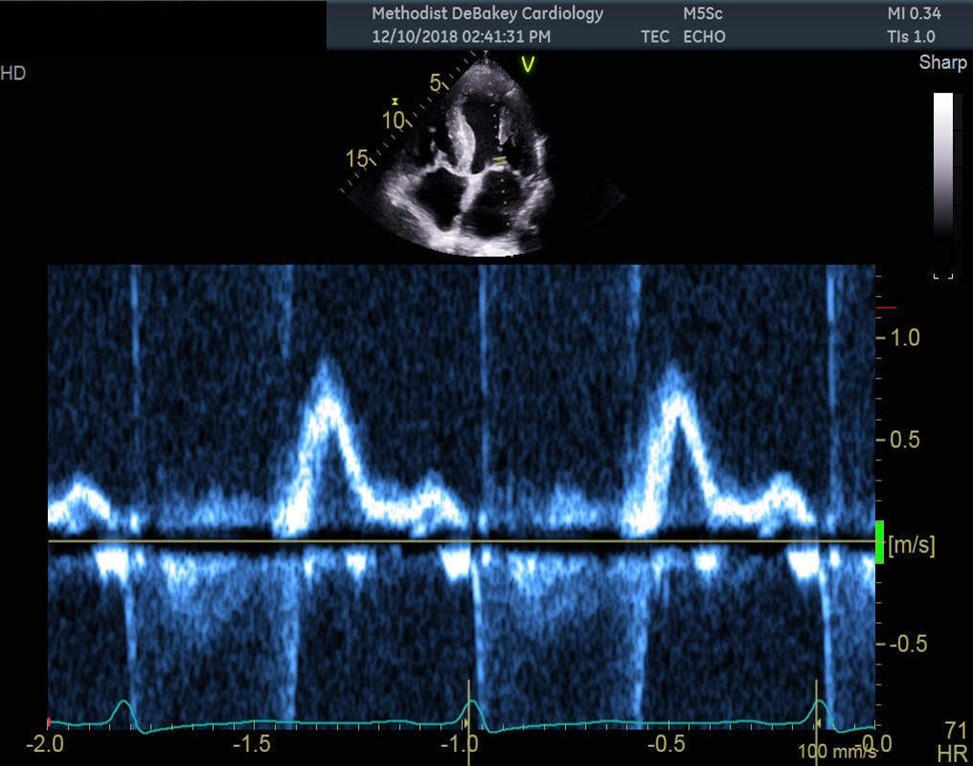
Figure 1: Pulsed-Wave Doppler at Mitral Valve Inflow
Figure 1
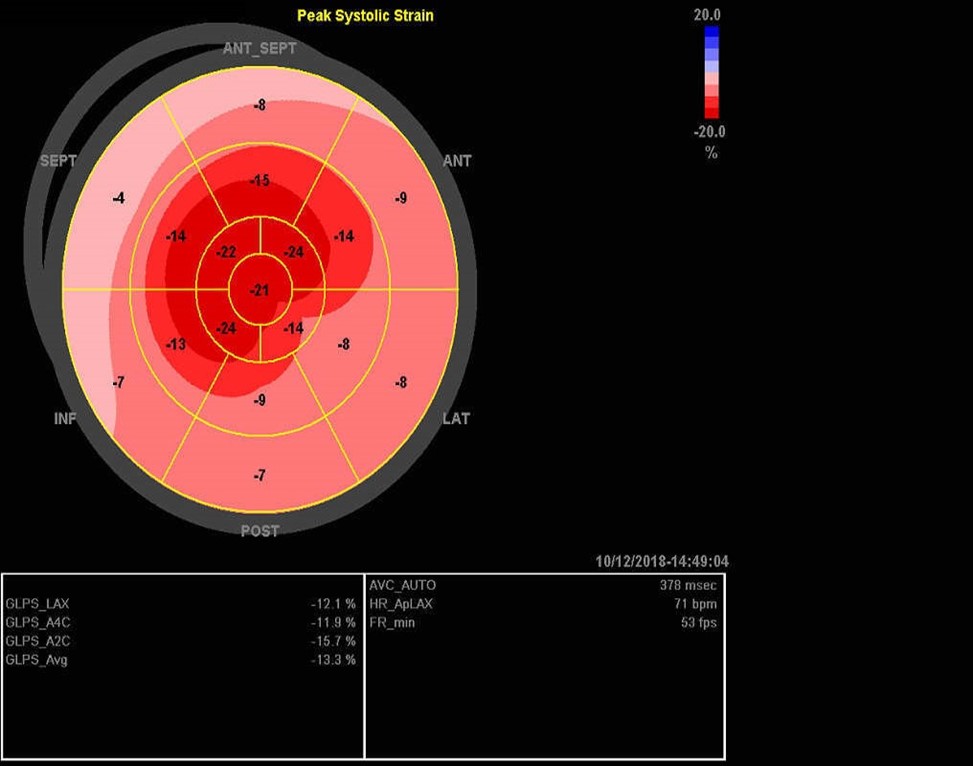
Figure 2: "Bullseye" Map of Left Ventricular Longitudinal Strain Pattern
Figure 2
Which one of the following is the appropriate next step in diagnosis?
Show Answer
The correct answer is: A. Technetium-99m (Tc-99m) pyrophosphate (PYP) scintigraphy.
The appropriate next step for diagnosis in this patient is Tc-99m PYP scintigraphy.1 Her sFLC ratio was within the reference range in the context of ESRD (0.54-3.3 in these patients).2 This finding is explained by understanding the production and clearance of sFLC. The bone marrow produces approximately twice as much κ as λ free light chains (FLCs). Furthermore, κ and λ FLCs are cleared proportionally by the reticuloendothelial system, but κ FLCs are cleared significantly more efficiently than λ FLCs by the kidneys. Consequently, the κ FLC level starts to rise as renal function deteriorates because the kidneys' more efficient κ FLC clearance can no longer compensate for the relatively higher κ FLC production by the bone marrow. This rise leads to a higher reference range for κ FLC levels and a higher sFLC ratio in patients with ESRD compared with those of patients with normal kidney function.3 The combination of unremarkable UIFE, SIFE, and sFLC has a >99% sensitivity for ruling out amyloid light chain cardiac amyloidosis (AL-CA).4 A Tc-99m PYP scan will show significant myocardial uptake of the tracer compared with the contralateral lung field if there is underlying transthyretin amyloidosis cardiac amyloidosis (ATTR-CA).
cMRI is excellent for tissue characterization of myocardial protein deposition. Evaluating for late gadolinium enhancement is feasible in patients with ESRD when using group II gadolinium-based contrast agents but should be done in consultation with a nephrologist and radiology team if the study is needed to diagnose cardiac amyloidosis (CA).5 A diffuse myocardial uptake pattern would further increase suspicion of CA but is not enough to make the appropriate diagnosis by itself. Bone marrow biopsy is helpful to exclude hematologic malignancy as a cause of elevated light chains in the setting of a monoclonal protein spike on serum protein electrophoresis/urine protein electrophoresis. Fat pad biopsy is an insensitive test for diagnosing ATTR-CA (sensitivity <50% for ATTR-CA compared with 84% for AL-CA), and would be an inappropriate next step in this case.6,7 Genetic testing should be performed after making the diagnosis of ATTR-CA to discriminate the wild-type form from familial forms.
The timely diagnosis of amyloid cardiomyopathy is often delayed.8 This patient had multiple "red flags" for system amyloidosis with cardiac involvement. These flags included a restrictive early filling pattern, apical sparing pattern on echocardiography, orthostatic hypotension, and history of lumbar stenosis. Other echocardiographic clues included ventricular hypertrophy with small left ventricular cavity size, interatrial septal thickening, and biatrial enlargement.9 Proceeding with evaluating for CA would be the appropriate first step because AL-CA is a medical emergency with potential long-term survival when diagnosed and treated promptly.7 ATTR-CA can now be treated with transthyretin stabilizers such as tafamidis to delay disease progression and reduce all-cause mortality and cardiovascular-related hospitalization rates compared with placebo; however, patients with estimated glomerular filtration rate <25 mL/min/m2 were excluded from the ATTR-ACT (Transthyretin Amyloidosis Cardiomyopathy Clinical Trial), and efficacy in this patient group is unknown.10
References
Kittleson MM, Ruberg FL, Ambardekar AV, et al.; Writing Committee. 2023 ACC expert consensus decision pathway on comprehensive multidisciplinary care for the patient with cardiac amyloidosis: a report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol 2023;81:1076-126.
Long TE, Indridason OS, Palsson R, et al. Defining new reference intervals for serum free light chains in individuals with chronic kidney disease: results of the iStopMM study. Blood Cancer J 2022;12:133.
Witteles RM, Liedtke M. Avoiding catastrophe: understanding free light chain testing in the evaluation of ATTR amyloidosis. Circ Heart Fail 2021;Mar 19;[ePub ahead of print].
Muchtar E, Gertz MA, Kyle RA, et al. A modern primer on light chain amyloidosis in 592 patients with mass spectrometry-verified typing. Mayo Clin Proc 2019;94:472-83.
Garcia Y, Collins AB, Stone JR. Abdominal fat pad excisional biopsy for the diagnosis and typing of systemic amyloidosis. Hum Pathol 2018;72:71-9.
Witteles RM, Liedtke M. AL amyloidosis for the cardiologist and oncologist: epidemiology, diagnosis, and management. JACC CardioOncol 2019;1:117-30.
Lane T, Fontana M, Martinez-Naharro A, et al. Natural history, quality of life, and outcome in cardiac transthyretin amyloidosis. Circulation 2019;140:16-26.
Saad JM, Ahmed AI, Anugula D, Han Y, Alfawara MS, Al-Mallah MH. It takes a village: multimodality imaging of cardiac amyloidosis. Methodist Debakey Cardiovasc J 2022;18:47-58.
Maurer MS, Schwartz JH, Gundapaneni B, et al.; ATTR-ACT Study Investigators. Tafamidis treatment for patients with transthyretin amyloid cardiomyopathy. N Engl J Med 2018;379:1007-16.