A 78-year-old woman with a medical history of hypertension, diabetes mellitus, and chronic kidney disease presents for evaluation of difficulty with walking and balance that started approximately 1 year earlier. She states that her symptoms are not related to pain with walking, but she experiences extreme fatigue and blurred vision after walking a few yards. She reports that these episodes occur three to four times weekly.
Her right arm blood pressure (BP) is 110/69 mm Hg and her left arm BP is 160/70 mm Hg. Femoral, popliteal, and pedal pulses are equal bilaterally. No focal neurologic deficits are appreciated. Dizziness with recurrence of her symptoms is reported with her head tilted posteriorly.
A carotid duplex ultrasound is performed, with images (Figures 1, 2, 3, 4, 5, 6, 7) obtained from the right common carotid artery (RCCA), right internal carotid artery (RICA), right external carotid artery (RECA), right vertebral artery (RVA), right subclavian artery (RSA), left common carotid artery (LCCA), and left vertebral artery (LVA).
Figure 1
Figure 1
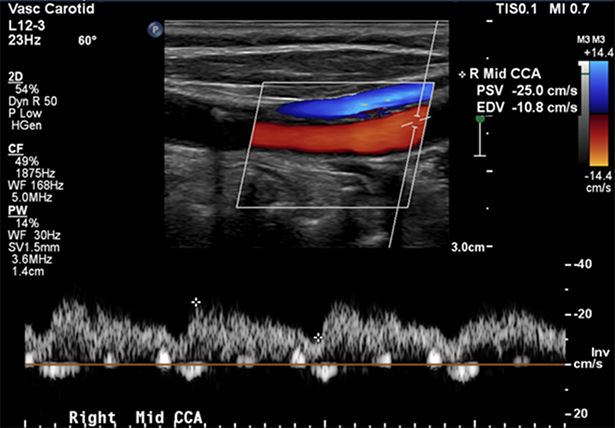
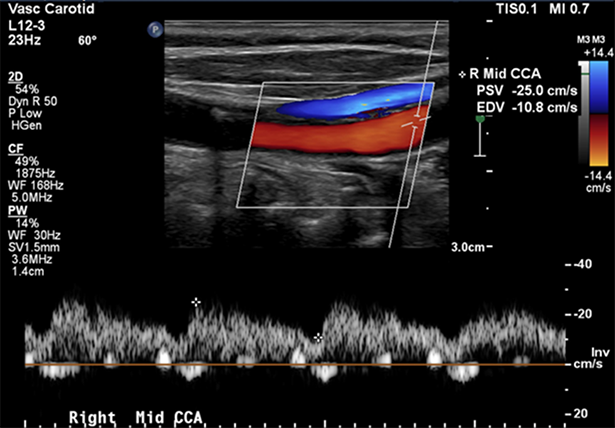
Longitudinal spectral Doppler ultrasound image of the RCCA.
Longitudinal spectral Doppler ultrasound image of the RCCA.
Figure 2
Figure 2
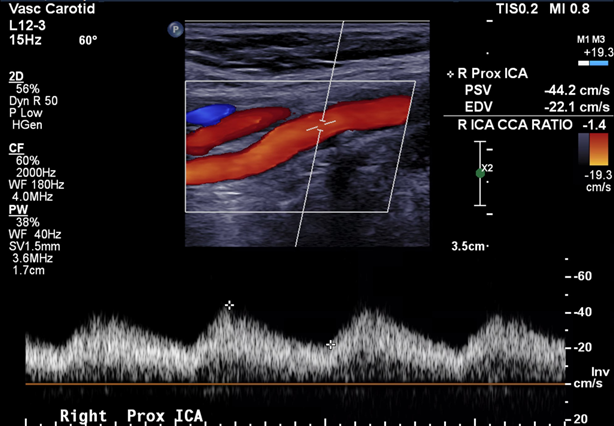
Longitudinal spectral Doppler ultrasound image of the RICA.
Longitudinal spectral Doppler ultrasound image of the RICA.
Figure 3
Figure 3
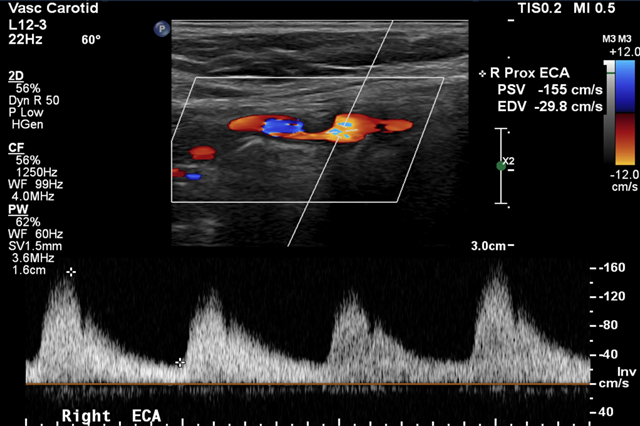
Longitudinal spectral Doppler ultrasound image of the RECA.
Longitudinal spectral Doppler ultrasound image of the RECA.
Figure 4
Figure 4
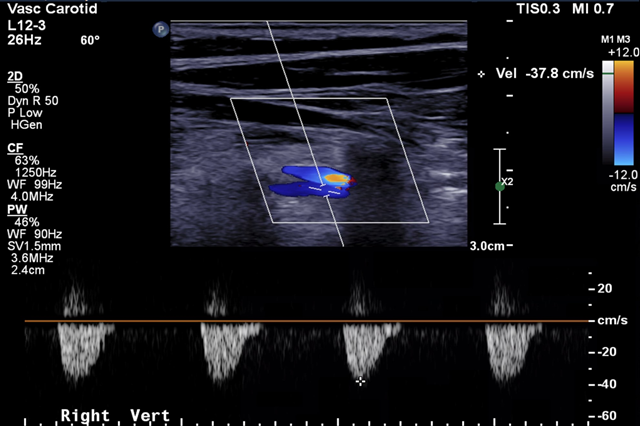
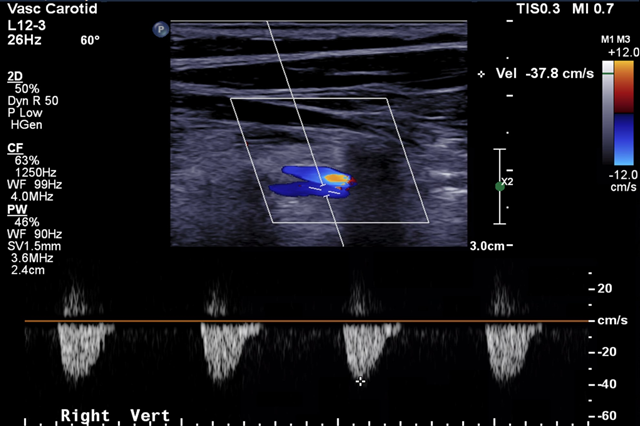
Longitudinal spectral Doppler ultrasound image of the RVA.
Longitudinal spectral Doppler ultrasound image of the RVA.
Figure 5
Figure 5
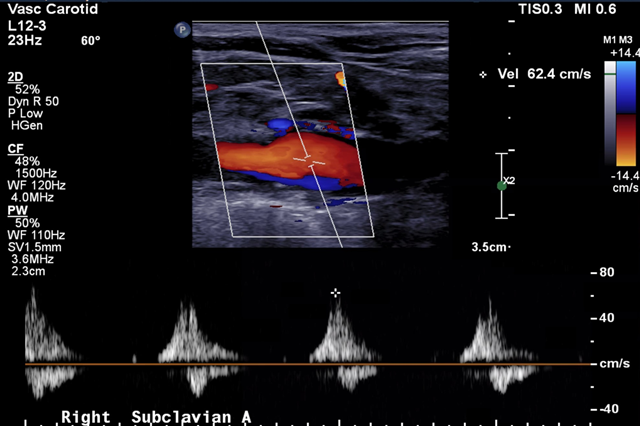
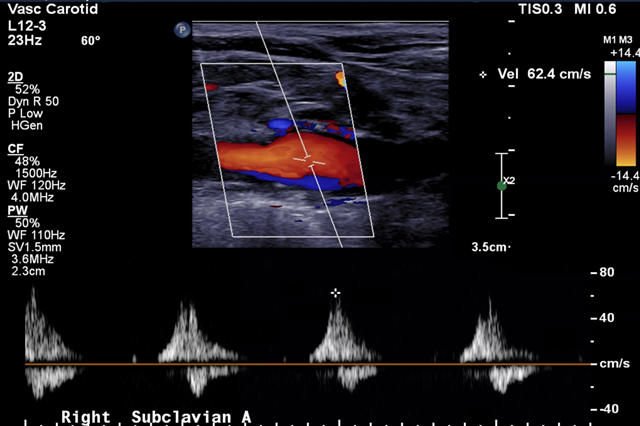
Longitudinal spectral Doppler ultrasound image of the RSA.
Longitudinal spectral Doppler ultrasound image of the RSA.
Figure 6
Figure 6
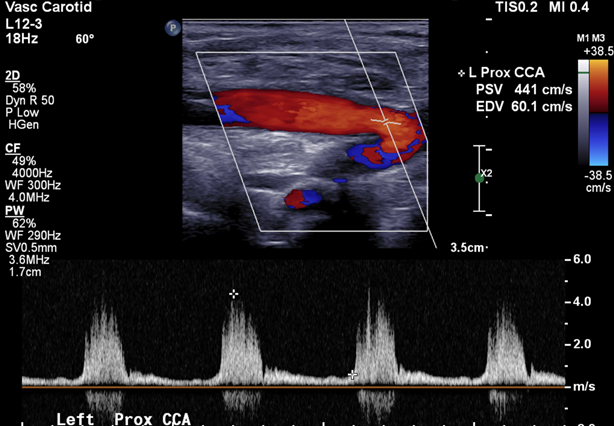
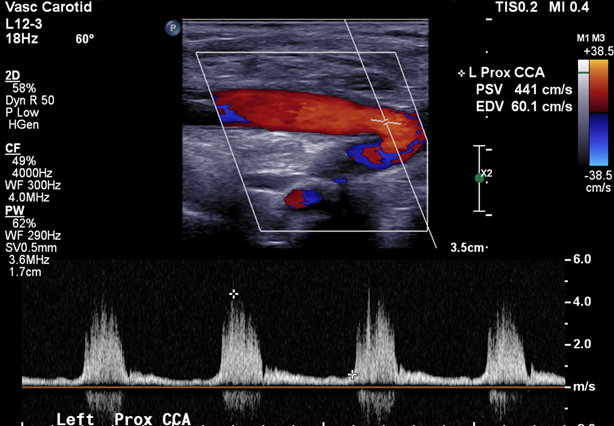
Longitudinal spectral Doppler ultrasound image of the LCCA.
Longitudinal spectral Doppler ultrasound image of the LCCA.
Figure 7
Figure 7
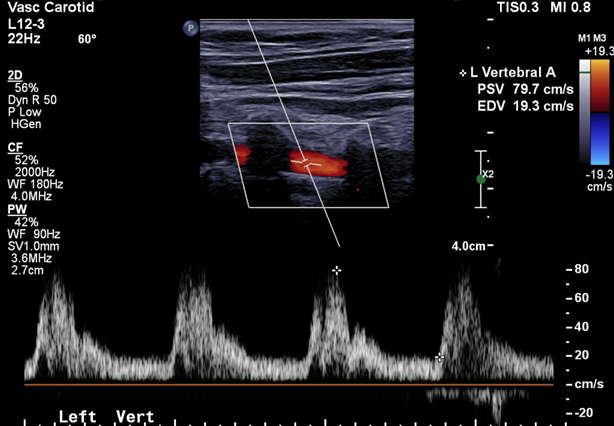
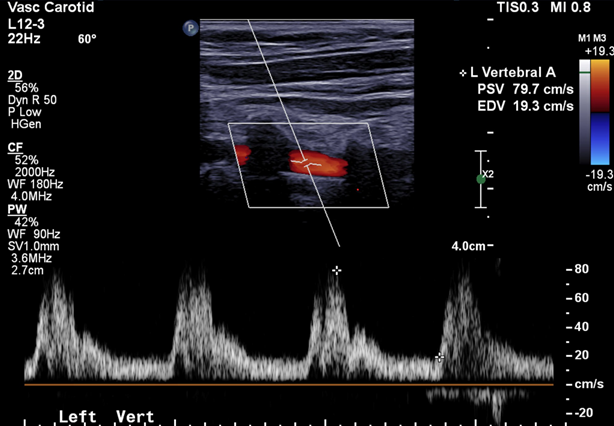
Longitudinal spectral Doppler ultrasound image of the LVA.
Longitudinal spectral Doppler ultrasound image of the LVA.
In which vessel is high-grade stenosis suspected?
Show Answer
The correct answer is: D. Brachiocephalic artery.
Interpretation of extracranial carotid duplex examination results should begin with the common carotid artery (CCA). Doing so will help ensure accuracy and consistency with reporting while providing details regarding the patency of the distal cerebrovascular system, contralateral cerebrovascular system, central vessels, and, in some cases, cardiac function.
The CCA should always be reviewed bilaterally. Peak systolic velocities within the CCA should measure within 30 cm/sec bilaterally. A velocity variance >30 cm/sec is indicative of a proximal obstruction, distal obstruction, vessel tortuosity, or compensatory flow.1
Unremarkable CCA Doppler waveform findings demonstrate rapid systolic upstroke and forward anterograde diastolic flow. Should the Doppler waveform demonstrate a delayed or prolonged systolic upstroke with a rounded systolic peak and reduced velocities unilaterally, a significant proximal obstructive lesion should be suspected in the side being observed.2 Cases in which the systolic waveform appears delayed or prolonged bilaterally are indicative of disease associated with the AoV. Suspected distal lesions are more apparent in the diastolic component of a waveform, a sign of increased vascular resistance or perfusion to a typically low-resistance bed.
It is anticipated and often observed that, in cases with unilateral obstructive lesions, the contralateral system compensates and provides additional perfusion, resulting in artificially high velocities. In such cases, special attention should be given to ensure the absence of plaque or turbulence within the distal segments of the vessel being investigated to ensure focal lesions are not overlooked.
In this case, the RCCA (Figure 1) demonstrated a prolonged systolic upstroke, forward diastolic flow, and velocity 25/10 cm/sec. The LCCA (Figure 6) demonstrated rapid systolic upstroke, forward diastolic flow, and velocity 441/60 cm/sec. This phenomenon resulted in velocity variance >30 cm/sec, indicating effects or disease within the right carotid system, which eliminated answer choices A and C. There was retrograde flow (reversed flow) in the RVA (Figure 4) and anterograde flow (forward flow) in the LVA (Figure 7). This finding indicated that flow within the RVA had reversed to help perfuse the right upper extremity, which was further supported by the BP gradient noted during physical examination. Monophasic Doppler signals were seen in the RSA (Figure 5), suggesting that the lesion was more proximal to the area being insonated. This finding eliminated answer choice B. As both the RCCA and RSA demonstrated impaired perfusion and altered Doppler waveforms, it was suspected that the source of disease was the brachiocephalic artery, which was the correct answer choice.
Figure 1
Longitudinal spectral Doppler ultrasound image of the RCCA.
Figure 4
Longitudinal spectral Doppler ultrasound image of the RVA.
Figure 5
Longitudinal spectral Doppler ultrasound image of the RSA.
Figure 6
Longitudinal spectral Doppler ultrasound image of the LCCA.
Figure 7
Longitudinal spectral Doppler ultrasound image of the LVA.
Kim ES, Sharma AM, Scissons R, et al. Interpretation of peripheral arterial and venous Doppler waveforms: a consensus statement from the Society for Vascular Medicine and Society for Vascular Ultrasound. Vasc Med 2020;25:484-506.