An 18-year-old man is seen in the cardiology clinic for evaluation of a murmur first noted during a recent sports physical examination. He reports occasional brief episodes of palpitations occurring at rest a few times per week. He denies exertional symptoms, chest pain, and syncope. He has no other significant medical conditions and his family history is unremarkable.
His physical examination findings are notable only for a midsystolic click and a harsh grade 3/6 late-peaking systolic regurgitant murmur best heard at the apex. An electrocardiogram (ECG) and transthoracic echocardiogram are performed (Figure 1; Videos 1, 2).
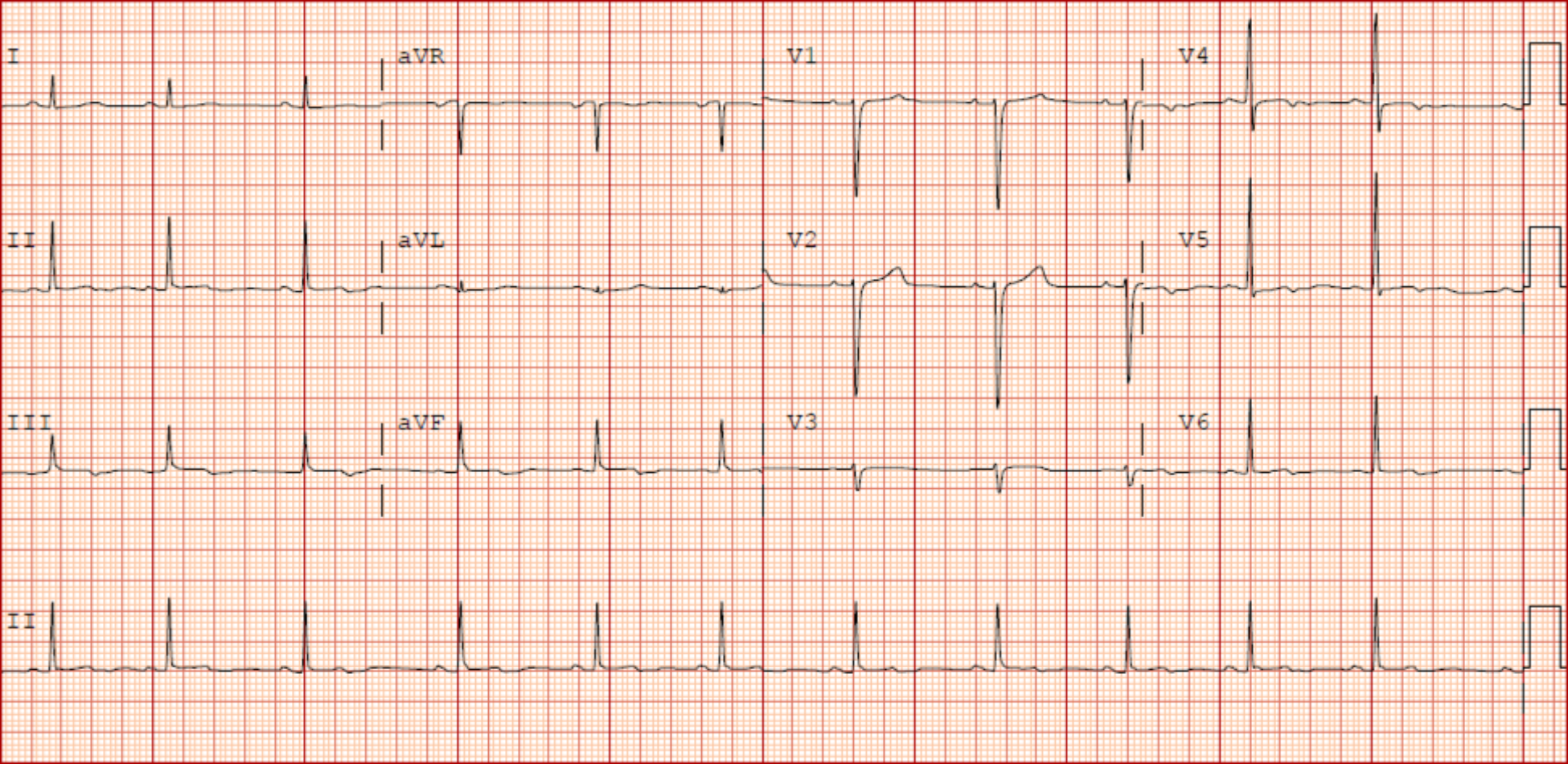
Figure 1: Twelve-Lead Electrocardiogram
Video 1: Echocardiogram
Parasternal long-axis view.
Video 2: Echocardiogram
Four-chamber view with color Doppler imaging of the mitral valve.
Which one of the following is the most appropriate next step in his management?
Show Answer
The correct answer is: B. Order ambulatory heart rhythm monitoring.
This patient's cardiac examination findings were remarkable, and his ECG findings included subtle T-wave abnormalities in the inferolateral leads. His echocardiogram revealed bileaflet mitral valve prolapse (MVP), mitral annular disjunction (MAD), and mitral regurgitation (MR). Given these findings, he may be at risk of a malignant arrhythmia. Ambulatory rhythm monitoring would be the most appropriate next step in management to evaluate for a pathologic arrhythmia given his report of palpitations and the need for sports clearance.
An invasive EPS would not be indicated without first identifying and characterizing rhythm abnormalities with ambulatory rhythm monitoring. A cardiology follow-up visit in 1 year might have been appropriate but further testing was indicated. A stress echocardiogram would not be indicated in this scenario for the evaluation of MVP and MAD.
MVP is often defined as atrial displacement of a mitral valve (MV) leaflet >2 mm from the mitral annulus in systole on parasternal long-axis imaging (Figure 2).
Figure 2: Systolic Frame From the Echocardiogram in Video 1 Showing a PLAX View
There is MVP with displacement of the MV leaflets 6 mm (blue bracket) from the plane of the MV annulus (red line). There is also a separation of the mitral annulus and LA wall from the LV myocardium of approximately 7 mm (green bracket), consistent with MAD.
LA = left atrial; LV = left ventricular; MAD = mitral annular disjunction; MV = mitral valve; MVP = mitral valve prolapse; PLAX = parasternal long-axis.
A classic definition also includes leaflet thickness >5 mm in diastole as a criterion, indicative of myxomatous MV degeneration.1 Typical examination findings include a midsystolic click, which may be present at baseline or provoked by isometric handgrip. If there is accompanying MR, a late systolic murmur best heard at the apex, typically accentuated by upright posture, may be present, as in this case.
The clinician is beset with numerous published reports describing the outcomes of patients with MVP, which range from a benign course to sudden cardiac death (SCD). Previous data have suggested several risk factors for SCD in patients with MVP, including myocardial fibrosis, MAD, complex ventricular ectopy, bileaflet MVP, moderate or greater MR, and female sex.2 A combination of the aforementioned factors can be encompassed by the terms arrhythmic mitral valve prolapse or malignant mitral valve prolapse, which, although variably defined, generally indicate a variant of MVP with a higher-risk profile.2-4
MAD is defined by separation of the mitral annulus and left atrial wall from the left ventricular (LV) myocardium (Figure 2). Some experts require a separation distance of ≥5 mm as a diagnostic criterion.5 Cardiovascular magnetic resonance (CMR) imaging can provide a more sensitive evaluation given the variability in location of MAD along the mitral annulus. CMR can also evaluate for myocardial fibrosis, sometimes located within the papillary muscles or along the lateral wall of the LV.6 Although often associated with MVP, MAD is increasingly considered a distinct entity with histopathologic underpinnings and clinical ramifications. Dejgaard et al. studied 116 patients (mean age 49 ± 15 years, 60% female) with MAD and found palpitations in 71% of patients and the occurrence of arrhythmic events in 12%. Interestingly, 22% of patients did not have concomitant MVP, which itself was not associated with arrhythmic events, suggesting MAD as an arrhythmogenic entity.7 Results from a more recent study evaluating 595 patients (mean age 61 ± 16 years; 47% female) showed that the 31% of patients in the cohort with MAD experienced a higher rate of arrhythmic events. However, a link to higher mortality rates was not established.8 The optimal approach to risk stratification for patients with MVP and MAD is unresolved. For patients with symptoms of palpitations and ECG abnormalities, frequent monitoring is warranted to evaluate for ventricular arrhythmias.9
References
Faletra FF, Leo LA, Paiocchi VL, et al. Morphology of mitral annular disjunction in mitral valve prolapse. J Am Soc Echocardiogr 2022;35:176-86.
Miller MA, Dukkipati SR, Turagam M, Liao SL, Adams DH, Reddy VY. Arrhythmic mitral valve prolapse: JACC review topic of the week. J Am Coll Cardiol 2018;72:2904-14.
Basso C, Iliceto S, Thiene G, Perazzolo Marra M. Mitral valve prolapse, ventricular arrhythmias, and sudden death. Circulation 2019;140:952-64.
Delling FN, Noseworthy PA, Adams DH, et al. Research opportunities in the treatment of mitral valve prolapse: JACC expert panel. J Am Coll Cardiol 2022;80:2331-47.
Wunderlich NC, Ho SY, Flint N, Siegel RJ. Myxomatous mitral valve disease with mitral valve prolapse and mitral annular disjunction: clinical and functional significance of the coincidence. J Cardiovasc Dev Dis 2021;8:9.
Mantegazza V, Volpato V, Gripari P, et al. Multimodality imaging assessment of mitral annular disjunction in mitral valve prolapse. Heart 2021;107:25-32.
Dejgaard LA, Skjølsvik ET, Lie ØH, et al. The mitral annulus disjunction arrhythmic syndrome. J Am Coll Cardiol 2018;72:1600-9.
Essayagh B, Sabbag A, Antoine C, et al. The mitral annular disjunction of mitral valve prolapse: presentation and outcome. JACC Cardiovasc Imaging 2021;14:2073-87.
Sabbag A, Essayagh B, Barrera JDR, et al. EHRA expert consensus statement on arrhythmic mitral valve prolapse and mitral annular disjunction complex in collaboration with the ESC Council on valvular heart disease and the European Association of Cardiovascular Imaging endorsed cby the Heart Rhythm Society, by the Asia Pacific Heart Rhythm Society, and by the Latin American Heart Rhythm Society. Europace 2022;24:1981-2003.