A 38-year-old man diagnosed with hypertrophic cardiomyopathy (HCM) presents for his annual physical examination. He was diagnosed with HCM 1 year earlier and started on metoprolol XL 25 mg daily. He reports continued breathlessness with exertion, chest pain, and lightheadedness. He used to play tennis but no longer enjoys being active because of his symptoms. He was previously offered septal myectomy but declined surgery because of his home and work demands.
His vital signs include heart rate (HR) 65 bpm and blood pressure (BP) 115/75 mm Hg. An echocardiogram obtained before his first office visit had findings of left ventricular ejection fraction (LVEF) 70%, increased basal anteroseptal wall thickness (17 mm), systolic anterior motion, and septal contact. The left ventricular outflow tract (LVOT) gradient was measured at 65 mm Hg.
The patient is initiated on mavacamten 5 mg daily and his metoprolol XL dosage is reduced to 12.5 mg daily.
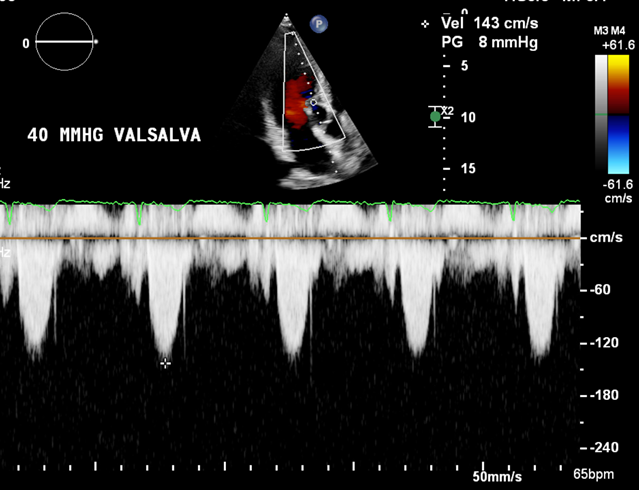
He presents for his 4-week repeat echocardiogram and office visit as outlined by the risk evaluation and mitigation strategy (REMS). He reports a modest improvement in exertional symptoms. His LVEF is 68% and LVOT gradient is 7 mm Hg at rest and 8 mm Hg with Valsalva (Figure 1).
Figure 1
The correct answer is: B. Reduce mavacamten to 2.5 mg daily and continue current metoprolol dose. Obtain a repeat echocardiogram in 4 weeks to guide dose titration.
This patient reported continued exertional symptoms despite beta-blocker (BB) therapy. His baseline HR was 65 bpm, preventing further uptitration of the BB. Because of his persistent symptoms and LVOT obstruction, adding a myosin inhibitor with mavacamten 5 mg in combination with an atrioventricular nodal (AVN) blocking agent would be recommended per the 2024 multisociety Guideline for the Management of HCM.1
Although this guideline recommends substitution of BB for a nondihydropyridine CCB, this class of medication also has the potential to elicit bradycardia in addition to hypotension from vasodilatory effects. Therefore, trialing CCB therapy would be unlikely to be tolerated. Similarly, escalation to disopyramide in addition to an AVN blocking agent would be unlikely to be tolerated.
Mavacamten is a cardiac myosin inhibitor that is effective in reducing LVOT gradients. Due to the potential to develop a systolic dysfunction with this class of medication, a REMS (similar to the dose titration schedule outlined in the VALOR-HCM [Mavacamten in Adults With Symptomatic Obstructive HCM Who Are Eligible for Septal Reduction Therapy] trial2), is required by the Food and Drug Administration (FDA) when placing patients on mavacamten. REMS requires close monitoring with repeat echocardiographic assessment at prespecified intervals to help detect left ventricular systolic dysfunction and direct dose titration. When there is a significant drop in LVEF to <50%, it is recommended to interrupt mavacamten therapy. In addition, when the LVOT gradient is <20 mm Hg in the first 4 weeks of therapy, it is recommended to reduce the dose of mavacamten to 2.5 mg and obtain a repeat echocardiogram in 4 weeks.
This patient case quiz is part of the larger Hypertrophic Cardiomyopathy: Accelerating Guideline-Driven Care grant. Educational grant support is provided by Bristol Myers Squibb. To visit the Hypertrophic Cardiomyopathy: Accelerating Guideline-Driven Care grant page and access additional educational activities on this topic, click here.
References
- Ommen SR, Ho CY, Asif IM, et al.; Writing Committee Members. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR guideline for the management of hypertrophic cardiomyopathy: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2024;83:2324-405.
- Desai MY, Owens A, Geske JB, et al. Myosin inhibition in patients with obstructive hypertrophic cardiomyopathy referred for septal reduction therapy. J Am Coll Cardiol 2022;80:95-108.
