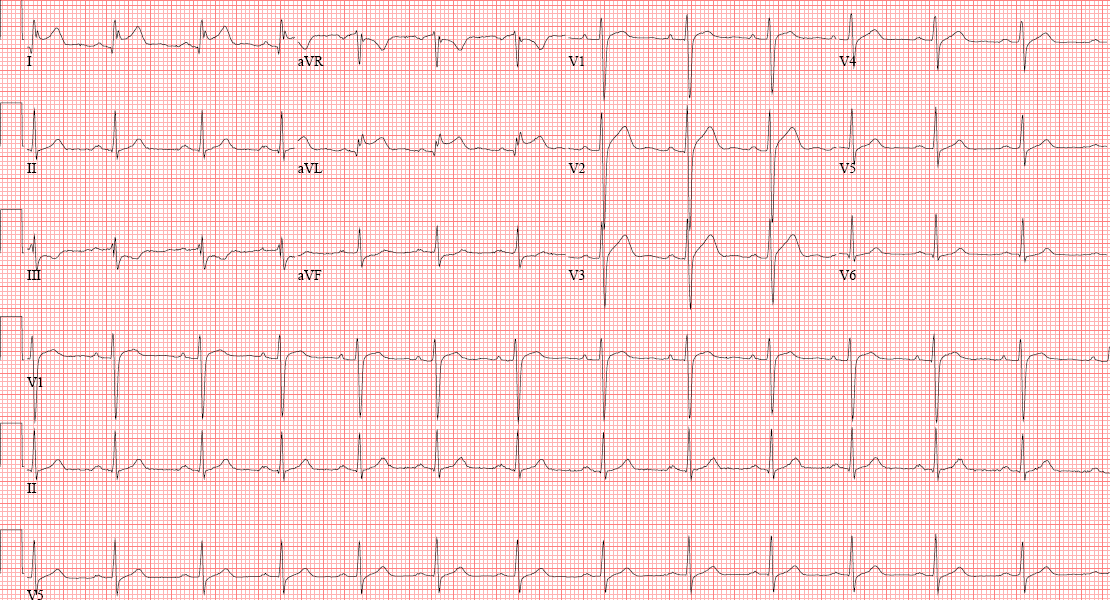
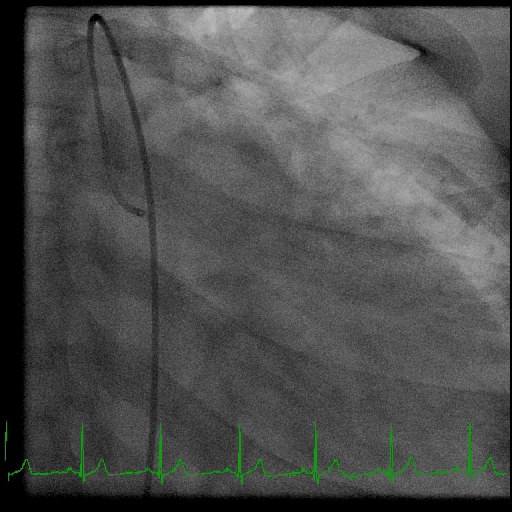
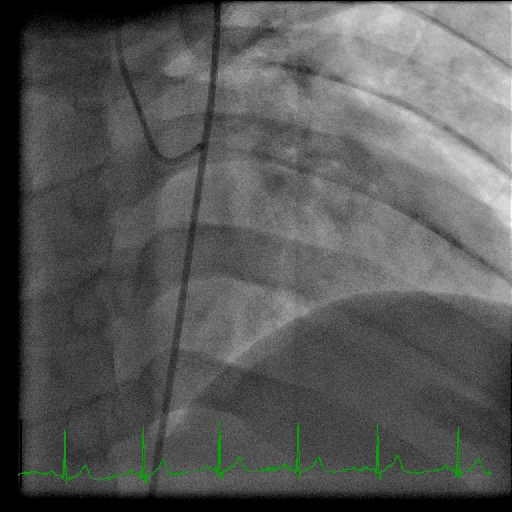
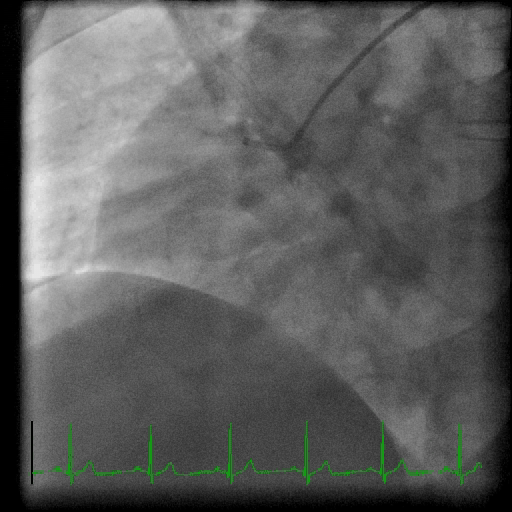
A 22-year-old male with no prior medical history presented to the Emergency Department with 2 days of intermittent chest discomfort. On arrival, his vital signs were unremarkable with a temperature of 98.3 oF, blood pressure 135/79 mmHg, pulse 91 beats/minute, respirations 12 breaths/minute, and SpO2 98% on room air. Blood pressure was equal in both upper extremities. Cardiovascular examination was within normal limits. Electrocardiogram (Figure 1) was notable for ST elevation in leads I and AVL with concomitant ST depression in leads III and AVF. Urine toxicology screen was negative. Cardiac catheterization laboratory was activated and patient was transferred for emergent coronary angiography. In the interim, initial troponin T resulted at 0.51 ng/mL (peak 0.7 ng/mL) with a CK-MB 30 ng/mL (peak 42 ng/mL). Coronary angiography demonstrated slow flow in the LAD with mild disease in the distal portion of the vessel (Figures 2a to 2d). Left ventriculography demonstrated a left ventricular ejection fraction (LVEF) of 45% and no significant aortic or mitral insufficiency. Left ventricular end-diastolic pressure was 16 mmHg. Inflammatory markers were markedly positive with an ultrasensitive CRP of 50 mg/L. ANA was negative. Cardiac MRI with delayed-enhancement imaging similarly revealed a LVEF of 48% in addition to sub-epicardial enhancement affecting the entire inferolateral and lateral walls with extension to the overlying pericardium (see Figure 3). Based upon the above findings, the patient was diagnosed with acute perimyocarditis and commenced on carvedilol, lisinopril, and low-dose ibuprofen, with instructions to restrict his exercise for 6 months. The patient has since done well from a cardiovascular perspective with normalization of his LVEF on follow up MRI and echocardiogram.
Figure 1: Presenting EKG demonstrating lateral ST elevation.
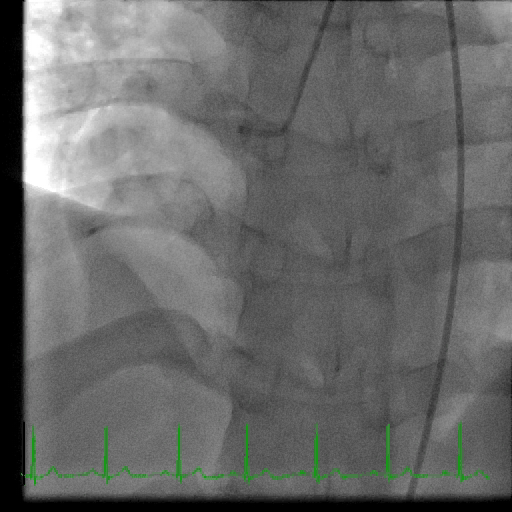
Figure 2a-2d: Coronary angiogram demonstrating the absence of any obstructive coronary artery disease.
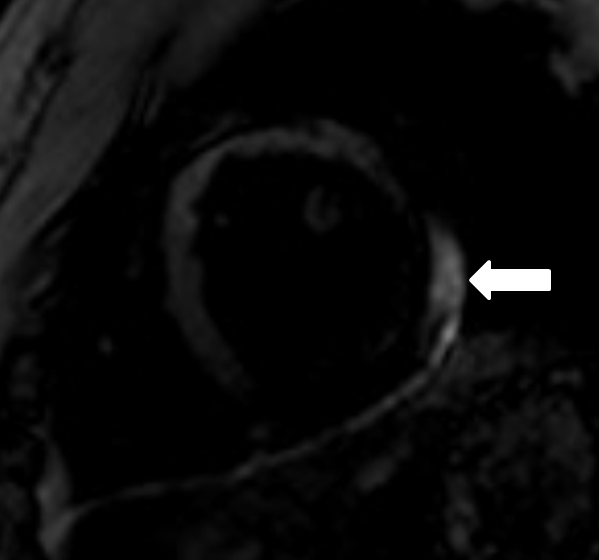
Figure 3: Cardiac MRI short axis sequence with gadolinium. Note the presence of focal delayed enhancement in the subepicardial portions of the lateral and inferolateral walls (see arrow).
What is the proposed mechanism for myocardial ischemia in patients such as the one above whose clinical presentation very closely resembles that of an acute myocardial infarction?
Show Answer
The correct answer is: C. Endothelial dysfunction and vasospasm
Among patients who present with acute pericarditis, troponin elevation can be seen in up to 35-50% of cases and is thought to reflect concomitant epicardial inflammation.1 The pattern of myocardial involvement is variable, with some cases being focal and others being more diffuse in nature.2 In a study conducted by Imazio et al. describing clinical features and outcomes involving 274 patients who presented with viral or idiopathic acute pericarditis, myocardial involvement was seen in 14.6% of cases, with approximately 6% of patients presenting initially with a presumed acute myocardial infarction.3 The patients with myocarditis tended to be younger, male, present with a febrile syndrome, and have atypical electrocardiographic features including focal ST elevations, arrhythmias and/or decreased ejection fraction. Although cases of fulminant cardiogenic shock with persistent heart failure are well-described in the literature, all but one patient had normalization of left ventricular function at 1 year follow up. In select cases where there is significant clinical concern for an acute myocardial infarction, coronary angiography is indicated as the initial means of evaluation. If a culprit lesion is not identified, one must consider alternate etiologies, including myocarditis. Among patients presenting with a clinical syndrome suggesting acute myocardial infarction with subsequent normal coronary angiography, endomyocardial biopsy-proven myocarditis has only been described in up to 34% of cases.4 Given the poor sensitivity of endomyocardial biopsy, cardiac MRI has now emerged as the diagnostic modality of choice in most patients owing to its ability to accurately assess left ventricular function, pattern and location of myocardial inflammation, as well as the extent of pericardial involvement.
Interestingly, cases involving parvovirus B19 appear to have a predilection for presenting along the clinical spectrum of an acute myocardial infarction.4-7 In a study of 87 patients with myocarditis, the group with parvovirus B19 (n=49) tended to present more commonly with severe acute chest pain , normal left ventricular ejection fraction, and focal late gadolinium enhancement in the subepicardial portion of the lateral left ventricular free wall.6 Although patients frequently experienced recurrent chest pain episodes within the first month following index presentation,, late recurrences were rare and left ventricular function tended to return to normal.
At the present time, it is unknown why cases of parvovirus B19 myocarditis tend to present in this manner. One hypothesis suggests that a combination of direct endothelial cell infection with resultant endothelial dysfunction and vasospasm may be the reason for this pattern.6, 8 Supporting this is the observation that coronary vasospasm could be directly induced by the use of intracoronary acetylcholine injection in 86% of patients with parvovirus B19 as compared to only 47% of patients with HHV6 myocarditis.8 In this study, the presence of parvovirus B19 infection was independently associated with coronary vasospasm on multivariate analysis.
When managing such patients, recognition of several specific disease phenotypes is important. The spectrum of acute myocardial and pericardial inflammatory syndromes varies from pure pericarditis to overlap syndromes with increasing myocardial involvement (myopericarditis and perimyocarditis) and finally to strict myocarditis. In patients with a diagnosis of acute pericarditis, the efficacy of combined therapy with NSAIDs and colchicine is well-established.9 With increasing myocardial inflammation and left ventricular dysfunction, attention must be paid to initiation and aggressive titration of guideline-directed medical therapy including ACE inhibitors and beta blockers to target doses. Such patients must also be counseled on exercise restriction for at least 4-6 weeks to minimize the risk of ventricular arrhythmias and be followed closely to determine the need for ICD implantation or in some cases evaluation for advanced therapies. Importantly, with increasing myocardial disease burden, the risk and benefit of NSAID therapy must be carefully weighed, owing to the observation that in animal models of myocarditis, NSAIDs were found to actually accelerate the inflammatory process and increase mortality.10
In summary, perimyocarditis is a common clinical entity among patients who present with presumed acute myocardial infarction and are subsequently found to have angiographically normal coronary arteries. The presumed mechanism is thought to represent a combination of endothelial dysfunction as well as vasospasm, with many cases involving the lateral wall of the left ventricle. Although the clinical course may be variable, most patients tend to have a benign course with full recovery of left ventricular function at long-term follow up.
References
Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004;35:2195-202.
Sarda L, Colin P, Boccara F, et al. Myocarditis in patients with clinical presentation of myocardial infarction and normal coronary angiograms. J Am Coll Cardiol. 200;37:786-92.
Imazio M, Cecchi E, Demichelis B, et al. Myopericarditis versus viral or idiopathic acute pericarditis. Heart. 2008;94:498-501.
Dec GW Jr, Waldman H, Southern J, et al. Viral myocarditis mimicking acute myocardial infarction. J Am Coll Cardiol. 1992;20:85-9.
Narula J, Khaw BA, Dec GW Jr, et al. Brief report: recognition of acute myocarditis masquerading as acute myocardial infarction. N Engl J Med. 1993;328:100-4.
Mahrholdt H, Wagner A, Deluigi CC, et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation. 2006;114:1581-90.
Kühl U, Pauschinger M, Bock T, et al. Parvovirus B19 infection mimicking acute myocardial infarction. Circulation. 2003;108:945-50.
Yilmaz A, Mahrholdt H, Athanasiadis A, et al. Coronary vasospasm as the underlying cause for chest pain in patients with PVB19 myocarditis. Heart. 2008;94:1456-63.
Imazio M, Brucato A, Cemin R, et al. A randomized trial of colchicine for acute pericarditis. N Engl J Med. 2013;369:1522-8.
Imazio M, Trinchero R. Myopericarditis: Etiology, management, and prognosis. International Journal of Cardiology. 2008;127:17–26.