A 31-year-old Caucasian female with history of hyperlipidemia who is an active smoker and is taking oral contraceptive pills for the last 10 years presented to the emergency department with constant substernal chest pain that started while jogging 3 hours prior to presentation. The chest pain was associated with numbness and tingling in the left arm; it was not related to position. She denied recent cough, fever, calf pain or swelling, or illicit drug use. Of note, the patient travels frequently to the West Coast for work. She has a strong family history of premature coronary artery disease (her brother had a myocardial infarction [MI] at age 40, and her mother had a coronary artery bypass graft at age 50).
Her physical exam was unremarkable with normal vital signs and no significant cardiac findings. Her initial electrocardiogram (ECG) showed normal sinus rhythm at 61bpm with nonspecific ST-T changes in the inferior leads and V3-V4. Initial troponin T and creatine kinase-myocardial band (CK-MB) were negative, and her white blood cell count was 20. Computed tomography angiogram of thoracic aorta was negative for dissection. The patient was given famotidine, an antacid, and acetaminophen, and her pain subsided. A repeat set of cardiac enzymes were positive, with troponin T of 1.03 and CK-MB of 54, and dynamic ST-T changes on a repeat ECG were noted in the inferior leads. The patient was admitted to the cardiac care unit for non-ST-segment elevation MI (NSTEMI) and started on aspirin, clopidogrel, low molecular weight heparin, rosuvastatin, and metoprolol. Transthoracic echocardiogram revealed a left ventricular ejection fraction of 60-65% and no regional wall motion abnormalities. The patient was taken to the cardiac catheterization laboratory with the results noted below.
Video 1
Video 2
Video 3
Video 4
What is the most likely diagnosis?
Show Answer
The correct answer is: C. NSTEMI
Following coronary angiogram that initially was interpreted as normal, the patient was referred for cardiovascular magnetic resonance (CMR) imaging for further evaluation of myocardial function and viability.
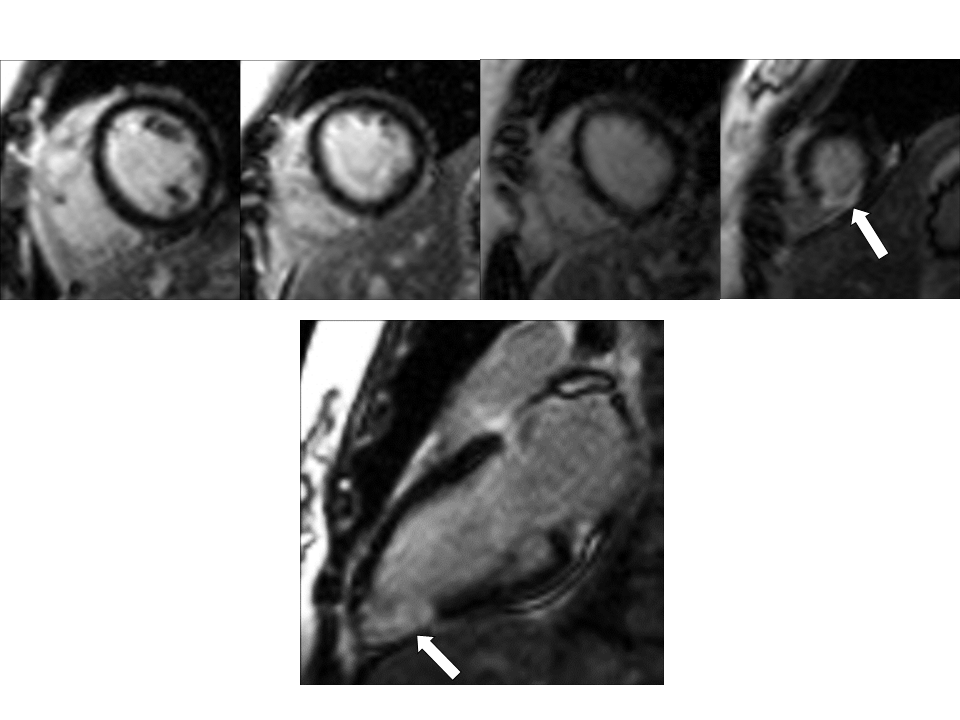
Figure 1: White arrows indicated a transmural inferoapical MI.
Video 1: Long axis two chamber steady-state free precession image (cine image) that shows akinesia of the apical inferior wall segment.
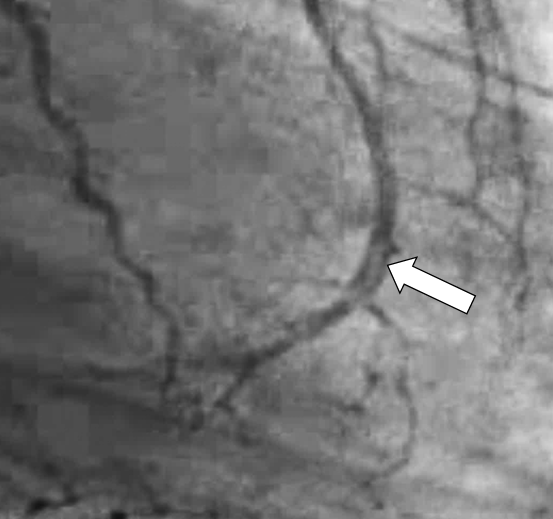
Following the results of the CMR exam, coronary angiography was reviewed again, and the distal left anterior descending artery was noted to have a thrombus present.
Video 2
Figure 2
Because neither intravascular ultrasound nor optical coherence tomography was performed at the time of the coronary artery angiography, we cannot determine the exact etiology of the thrombus. The differential includes rupture of a native atherosclerotic plaque with thrombosis formation, spontaneous coronary artery dissection, and embolization from an unknown source.
Based on previous studies, 25-37% of the patients presenting with acute chest pain and elevated troponins do not have identifiable infarct-related artery by coronary angiography.1,2 Larson et al. reported up to 14% of these patients had normal coronaries, and 9% had no significant coronary artery disease.3 Recently, late gadolinium enhancement by CMR became the gold standard for detection of scar associated with MI and other nonischemic causes.4 Three previous studies evaluating patients presenting with NSTEMI and no significant obstruction on coronary angiography found a late gadolinium enhancement pattern consistent with an acute MI in 11%, 30%, and 44% of the patients.4-6 One of these studies demonstrated a more than threefold increase in cardiac events on follow-up in those patients who had an acute MI pattern on late gadolinium enhancement CMR.5
This case demonstrates the potential utility of CMR in patients presenting with NSTEMI with no significant obstruction on coronary angiography. Although this patient clearly had a thrombus noted in the distal left anterior descending, this was only detected after the information from the CMR showed the interpreter where to look.
References
Kerensky RA, Wade M, Deedwania P, Boden WE, Pepine CJ, Veterans Affairs Non-Q-Wave Infarction Strategies in-Hospital (VANQWISH) Trial Investigators. Revisiting the culprit lesion in non-Q-wave myocardial infarction. Results from the VANQWISH trial angiographic core laboratory. J Am Coll Cardiol 2002;39:1456-63.
McCullough PA, O'Neill WW, Graham M, et al. A prospective randomized trial of triage angiography in acute coronary syndromes ineligible for thrombolytic therapy. Results of the medicine versus angiography in thrombolytic exclusion (MATE) trial. J Am Coll Cardiol 1998;32:596-605.
Larson DM, Menssen KM, Sharkey SW, et al. "False-positive" cardiac catheterization laboratory activation among patients with suspected ST-segment elevation myocardial infarction. JAMA 2007;298:2754-60.
Assomull RG, Lyne JC, Keenan N, et al. The role of cardiovascular magnetic resonance in patients presenting with chest pain, raised troponin, and unobstructed coronary arteries. Eur Heart J 2007;28:1242-9.
Christiansen JP, Edwards C, Sinclair T, et al. Detection of myocardial scar by contrast-enhanced cardiac magnetic resonance imaging in patients with troponin-positive chest pain and minimal angiographic coronary artery disease. Am J Cardiol 2006;97:768-71.
Codreanu A, Djaballah W, Angioi M, et al. Detection of myocarditis by contrast-enhanced MRI in patients presenting with acute coronary syndrome but no coronary stenosis. J Magn Reson Imaging 2007;25:957-64.