A 50-year-old African-American female presents to the emergency department with a 6-hour history of worsening left-sided chest and back pain. Chest pain is described as a moderate intensity, constant, sharp pain which is present at rest and is not worsened by activity. She has a 20 pack/year smoking history. Her mother was diagnosed with coronary artery disease at age 50. Her blood pressure is 130/70 Electrocardiogram shows sinus rhythm with no evidence of ST or T wave abnormalities. Serial troponins are negative. Hemoglobin A1c is 6. Total cholesterol 180, HDL 30, LDL 140. Chest X-ray is normal with no evidence of mediastinal widening, no lung infiltrates and no evidence of pulmonary vascular congestion. Her chest pain does not improve with sublingual nitroglycerin, but resolves with gastrointestinal cocktail.
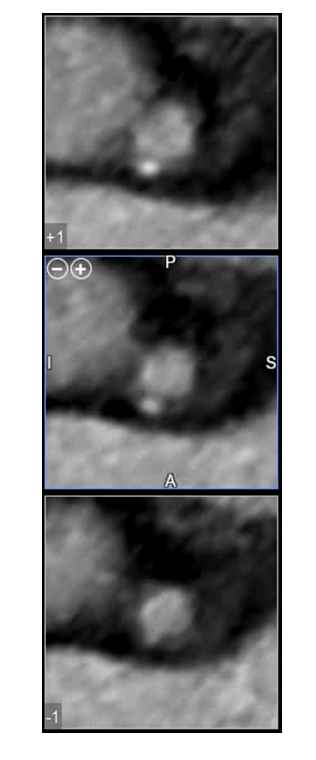
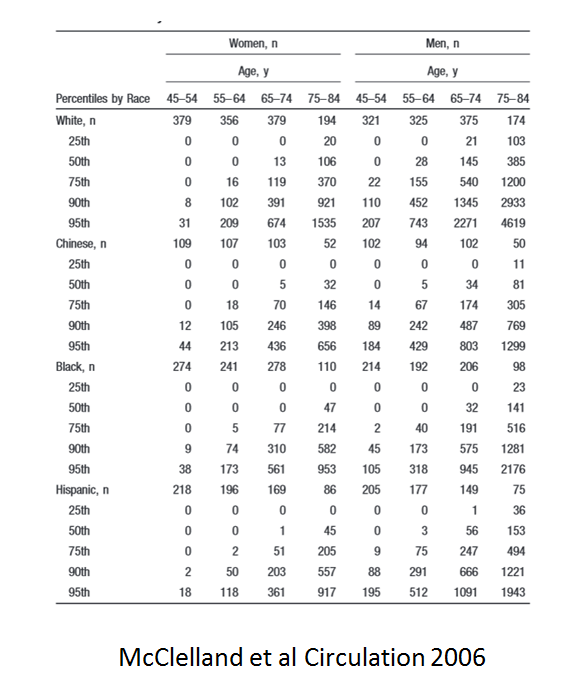
A coronary CT angiogram is ordered which showed a left dominant system and evidence of non-obstructive plaque (figures I-III). Coronary calcium score is 189, which is > 95th percentile for age/gender/race (see table 1). Her Segment Involvement Score (SIS) is 3, Segment Stenosis Score (SSS) is 0 and CT-Leaman Score (CT-LeSc) is 9 Smoking cessation is recommended.
She requests your recommendations about her long-term risk for cardiac death and non-fatal acute coronary syndrome compared to a person with no coronary plaque:
Show Answer
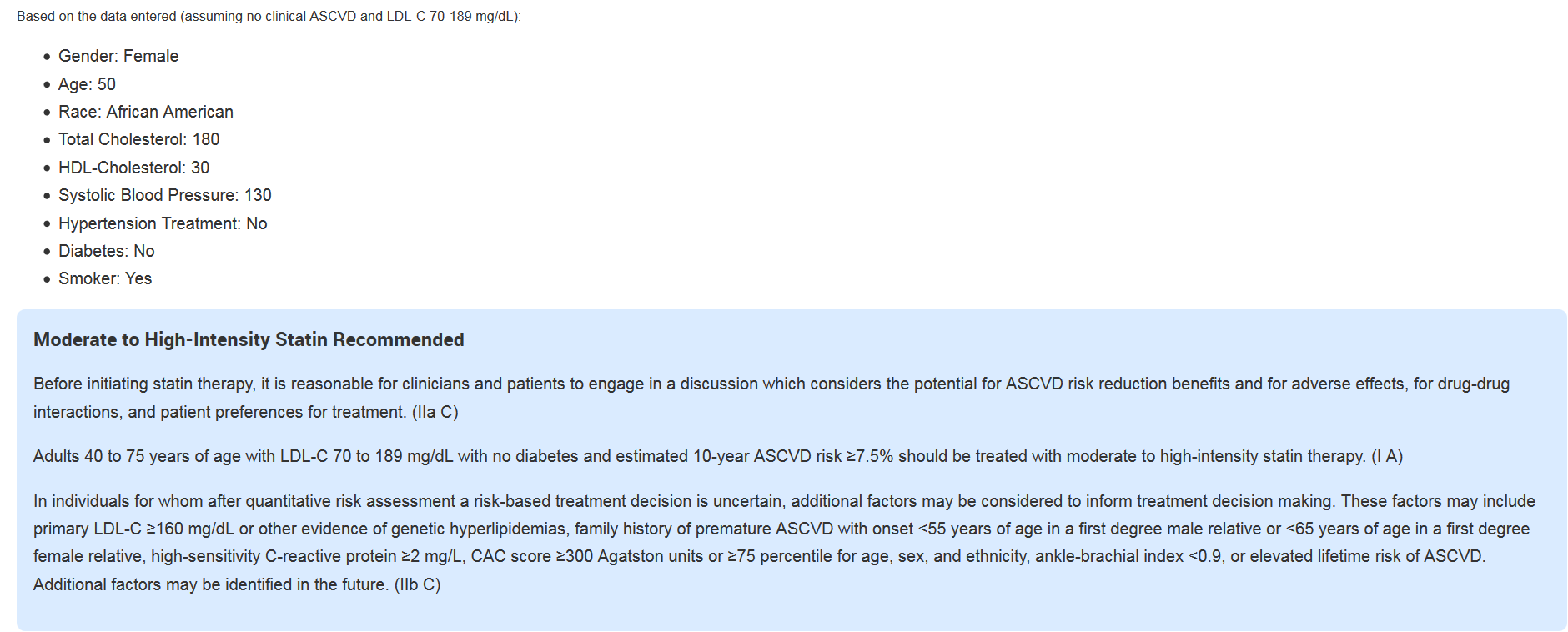
The correct answer is: B. Primary prevention estimated 10-year ASCVD risk ≥7.5%, statin therapy recommended
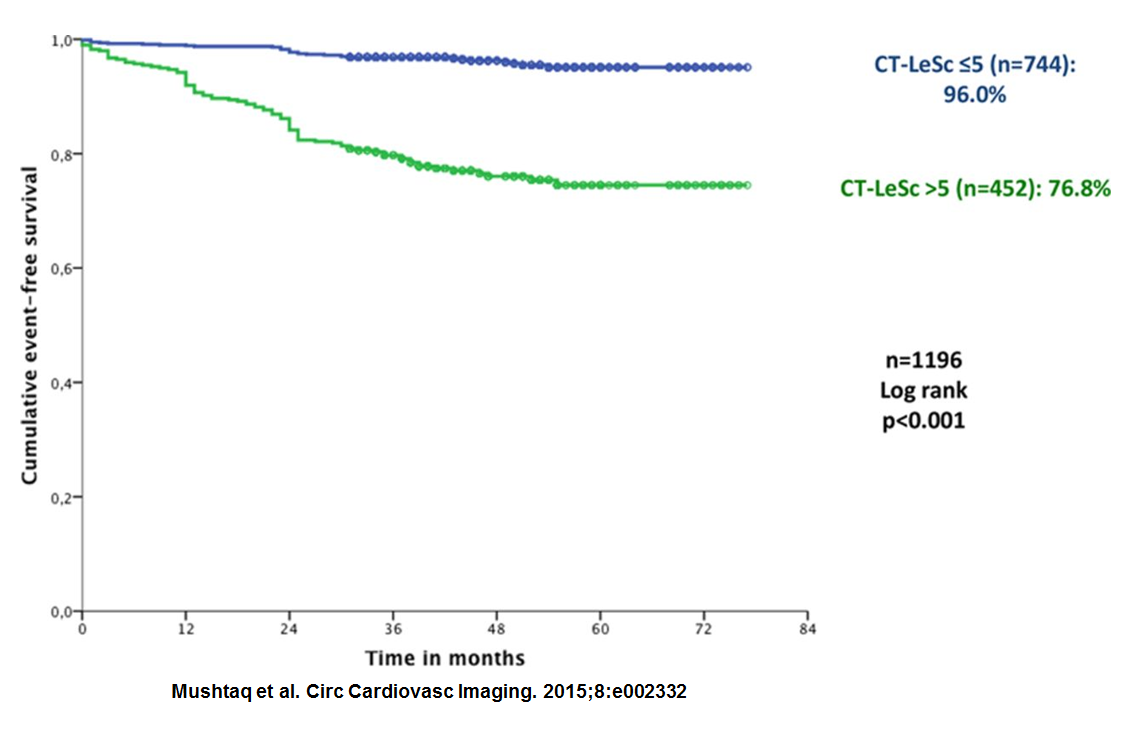
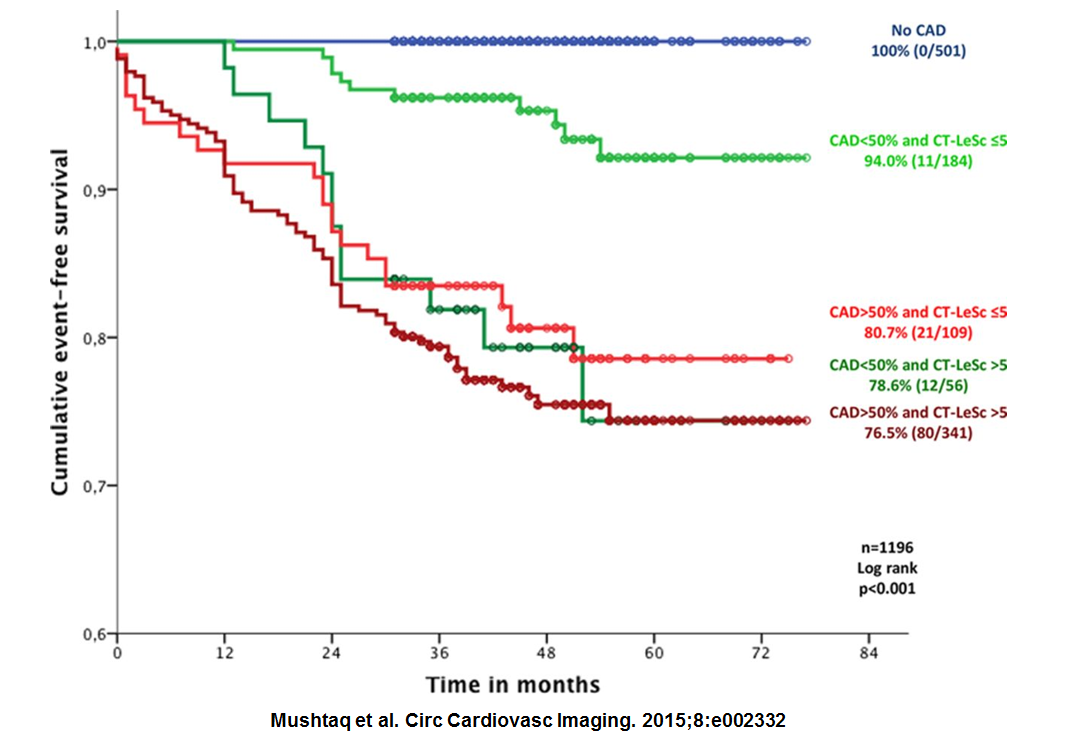
The Computed tomography-adapted Leaman score (CT-LeSc) is an atherosclerotic burden score which utilizes lesion localization, stenosis degree and plaque composition. Two other atherosclerotic burden scores: Segment Stenosis Score (SSS) and Segment Involvement Score (SIS) have previously been shown to predict long-term prognosis in patients with suspected coronary artery disease (CAD). 1 A single-center prospective registry study was recently performed to evaluate the long-term prognostic value of the CT-Leaman score (an atherosclerotic burden score) for hard cardiac events in 1304 patients. 2 The long-term prognostic value of the SSS and SIS for hard cardiac events, was also evaluated. Four tertiles of patients were identified: non-obstructive CAD (< 50% stenosis) and low CT-LeSc (≤5), non-obstructive CAD and high CT-LeSc (>5), obstructive CAD and low LeSc (≤5) and obstructive CAD and high LeSc (>5). After a mean follow-up period of 52 ± 22 months, 136 hard events occurred in 125 patients. The results showed that all three atherosclerotic burden scores were independent predictors of cardiac events: hazard ratio 3.09 for SIS, 4.42 for SSS and 5.39 for CT-LeSc. Patients with CT-LeSc scores ≤ 5 had a higher event free survival compared to patients with CT-LeSc scores> 5 (Figure IV). Event free survival was highest in patients with normal coronary arteries (100%), followed by patients with non-obstructive CAD and a low CT-LeSc ≤ 5 (94%) and patients with obstructive CAD and low CT-LeSc (80.7%). Event free survival was similar for patients with obstructive CAD and a high CT-LeSc (76.5%) and patients with non-obstructive CAD with high CT-LeSc (78.6%) [Figure V]. Based on this study, our patient with non-obstructive coronary artery disase and a high CT-LeSc score >5 would have a hard cardiac event rate similar to a patient with obstructive CAD and a high CT-LeSc score >5.
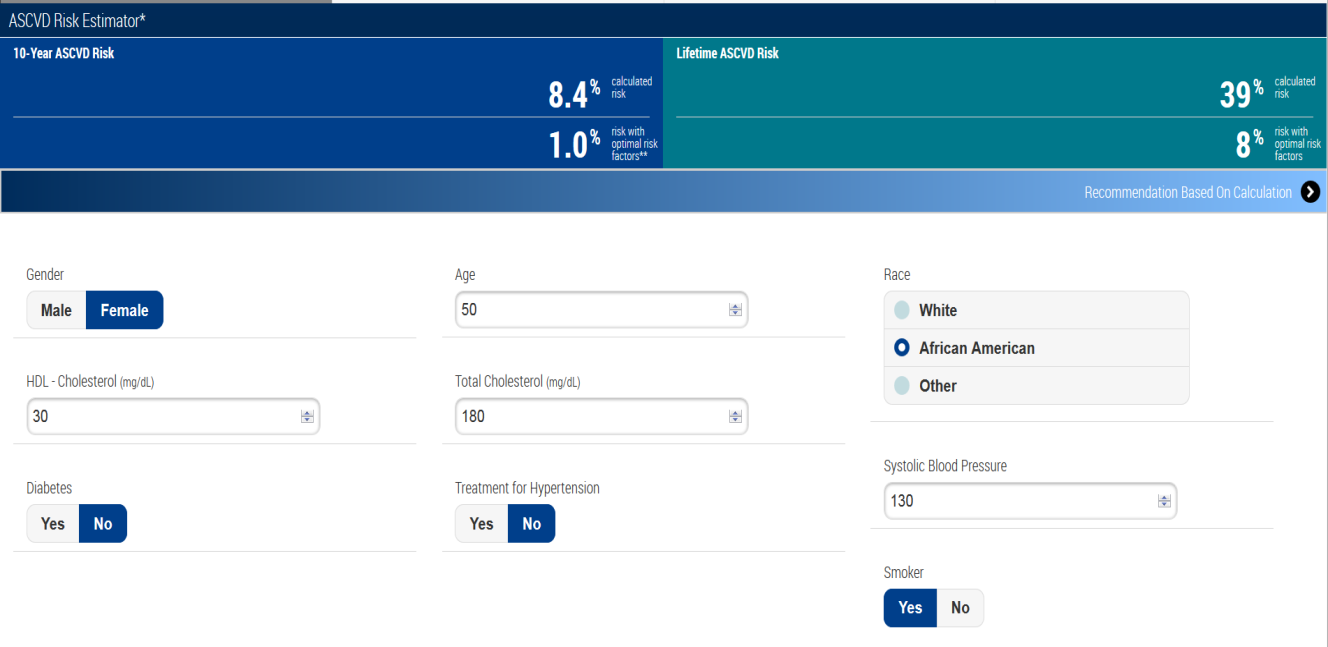
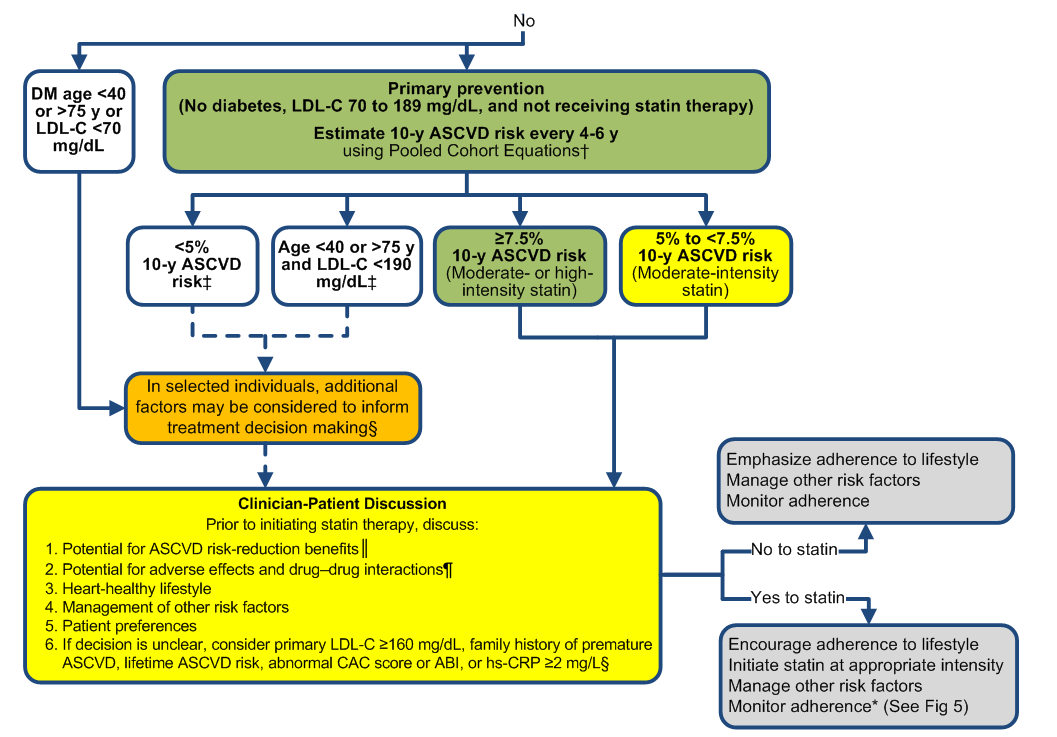
This patient's chest pain is unlikely cardiac in origin. However, she belongs to the statin benefit group of "No Diabetes; ≥7.5% 10-year ASCVD risk, age 40-75 years, LDL-C 70-189 mg/dL" as identified by the 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 3. Using the ASCVD risk calculator, her 10-year atherosclerotic risk for cardiovascular disease is 8.4% and 39% ASCVD lifetime risk (figures VI and VII). She does not have clinical atherosclerosis which is defined as acute coronary syndromes, history of MI, stable or unstable angina, coronary or other arterial revascularization, stroke, TIA, or peripheral arterial disease presumed to be of atherosclerotic origin. Initiation of a moderate or high intensity statin is a Class IA guideline recommendation. A clinician-patient discussion should be held to review the risks and benefits of statin therapy.
Her Agatson score is above the 90th percentile for her age, gender and race 4 and she has a family history of early coronary artery disease. A recent analysis of the Framingham cohorts found the >7.5% 10-year ASCVD risk cut-point to perform better than ATP III-based cut-points for identifying high risk patients likely to benefit from statin therapy, and the presence of CAC>0 further refined the identification of those at the highest ASCVD risk 5. An accompanying cost-effectiveness analysis also found the >7.5% 10-year ASCVD risk cut-point to be cost effective compared to a >10% 10-year ASCVD risk cut-point 6.
Options 'A' and 'D' are incorrect. She does not have features of clinical ASCVD as defined in the 2013 ACC/AHA cholesterol guideline based on the randomized trial inclusion criteria. No cardiovascular outcomes cholesterol treatment trial to date has used CAC scoring as eligibility criteria. Based on the 2013 ACC/AHA cholesterol guidelines, a coronary artery calcium score ≥ 300 Agaston units may help inform clinical decision making in patients who do not belong to a statin benefit group and in whom risk decision is uncertain. Option "E" is incorrect. Given her 10-year calculated ASCVD risk, statin therapy is recommended (Class I level of evidence A guideline recommendation). The long-term prognostic role of coronary CTA remains an area of interest.
Figure I: Coronary CTA showing LAD with calcified plaque (yellow arrow). Plaque in LCX (red arrow) and LM (blue arrow) can also be seen
Figure II: Coronary CTA showing calcification in the proximal circumflex artery
Figure III: Coronary CTA short axis images of left main artery showing mixed plaque with both calcification and non-calcified plaque
Figure IV: Kaplan-Meier survival curves for hard cardiac events stratified by coronary atherosclerotic burden (CT-LeSc >5 vs ≤5)
Figure V: Kaplan-Meier survival curves for hard cardiac events stratified by CAD severity (obstructive vs non-obstructive) and coronary atherosclerotic burden (CT-LeSc >5 vs ≤5)
Figure VII: Summary of Statin Initiation Recommendations to Reduce ASCVD Risk
Table I: Estimated Percentiles of CAC by Age Category, Gender, and Race/Ethnicity
References
Andreini D et al. A long-term prognostic value of coronary CT angiography in suspected coronary artery disease. JACC Cardiovasc Imaging 2012;5:690 –701
Mushtaq, S., et al., Long-term prognostic effect of coronary atherosclerotic burden: validation of the computed tomography-Leaman score. Circ Cardiovasc Imaging 2015; 8:e002332.
Stone, N.J., et al., 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; 63: 2889-934.
McClelland, R.L., et al., Distribution of coronary artery calcium by race, gender, and age: results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation 2006; 113: 30-7.
Pursnani, A., et al., Guideline-Based Statin Eligibility, Coronary Artery Calcification, and Cardiovascular Events. JAMA 2015; 314: 134-41.
Pandya, A., et al., Cost-effectiveness of 10-Year Risk Thresholds for Initiation of Statin Therapy for Primary Prevention of Cardiovascular Disease. JAMA 2015; 314: 142-50.