The patient is a 51-year-old man with history of hypertension and hyperlipidemia who presented with several weeks of progressive fatigue and four days of shortness of breath, dyspnea on exertion, orthopnea, and lower extremity edema. He was diagnosed by history and examination with congestive heart failure. Transthoracic echocardiography left ventricular dilatation (end-diastolic internal dimension 6.7 cm) with severe global systolic dysfunction (EF 22%), severely depressed right ventricular function, a severely dilated left atrium, and moderate mitral regurgitation. Right heart catheterization showed elevated filling pressures, with a pulmonary arterial occlusion pressure of 31 mmHg, and depressed cardiac index of 1.8 L/min/m2. Coronary angiography showed 20% stenosis of the mid-LAD and no other significant epicardial coronary disease. Cardiac MRI showed a small focal endocardial area of delayed gadolinium enhancement in the mid-inferior wall.
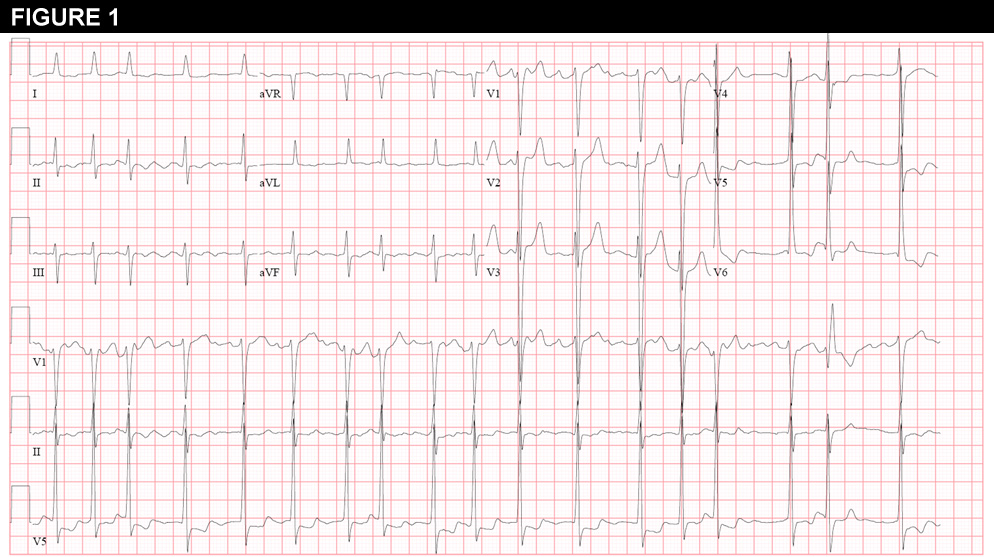
He was treated for newly diagnosed non-ischemic cardiomyopathy and congestive heart failure with aggressive afterload reduction and diuresis, and he was discharged on hospital day 4 in good condition. He presented to the clinic 2 weeks later with increasing exertional fatigue, intermittent nausea, and “agitation.” He denied chest discomfort or palpitations. The EKG from the clinic visit is shown in Figure 1.
He was admitted for initiation of anticoagulation and TEE-guided cardioversion, performed without complication. He was discharged on enoxaparin and warfarin. Symptomatic atrial fibrillation recurred within one week, and amiodarone therapy was initiated. A second cardioversion was performed, again with early recurrence of symptomatic atrial fibrillation. After a discussion of the potential risks and benefits, he was referred for pulmonary vein isolation.
The patient remained on warfarin, and on the morning of the procedure the following studies were obtained:
Laboratory Values:
Table: Laboratory Values
Sodium: 138
(134 - 149 mEq/L)
WBC: 9.0
(3.5 - 11 x103/uL)
Potassium: 4.1
(3.3 - 4.7 mEq/L)
Hgb: 13.9
(13.5 - 17.5 g/dL)
Serum creatinine: 1.3
(0.5 - 1.4 mg/dL)
Platelets: 305
(150 - 450 x103/uL)
Magnesium: 2.2
(1.6 - 2.5 mg/dL)
PT: 24.6
(12.1 - 14.9 secs)
INR: 2.1
(0.9 - 1.1)
Transesophageal Echocardiogram:
Left ventricular performance severely reduced. Right ventricular performance moderately reduced. No intracardiac mass or thrombus, but spontaneous echo contrast noted in the left atrium. Mitral annular dilation with moderate-severe mitral regurgitation. Mild-moderate tricuspid regurgitation.
Electrophysiology Procedure:
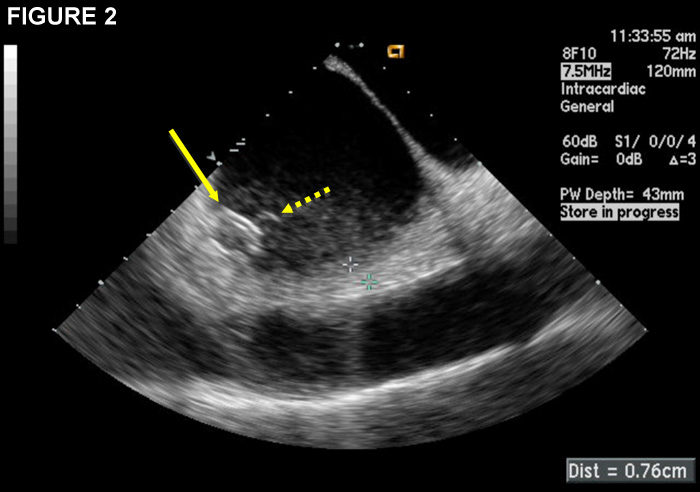
Heparin bolus and continuous infusion was administered prior to double transseptal puncture to achieve an activated clotting time (ACT) >350 seconds (secs). During electroanatomic mapping, the ACT was noted to have fallen to 260 secs. Intracardiac echocardiographic (ICE) imaging from that time is shown in Figure 2 and the accompanying video.
Based on the above information and findings, the next best step in management would be:
Show Answer
The correct answer is: B. Intensify anticoagulation with additional heparin
Figure 2 shows a linear thrombus (dashed arrow) attached to the circular mapping catheter (solid arrow) in the left atrium. The highly mobile thrombus can be seen clearly attached to the catheter (green circle) in the video. Given the relatively low ACT at the time the thrombus was discovered, intensifying anticoagulation to a goal ACT >350 secs will help prevent further thrombus formation and potentially enhance dissolution of the thrombus while preparations are made for more definitive management.
Though infrequent, thromboembolic stroke is a dreaded complication of left atrial ablation for treatment of atrial fibrillation. In a widely cited worldwide survey of 181 centers performing ablation procedures for atrial fibrillation, the incidence of ischemic cerebrovascular events was 0.94% among the 7,154 patients who underwent intervention in the left atrium.(1) However, maintenance of a therapeutic INR at the time of the procedure was not commonly practiced at that time. Furthermore, while all surveyed centers administered heparin during the procedure, minimum ACT targets were between 230 to 350 secs (if ACT guidance was used at all). Aspirin alone was administered post-procedure in 17% of centers.
Since then, a number of investigators have reported experience with ablation for atrial fibrillation while on therapeutic anticoagulation with warfarin.(2-7) With the exception of one study, the incidence of ischemic cerebrovascular events in patients with a therapeutic INR was lower than that reported by Cappato et al, with zero events reported in several studies.(2,5,6) In the largest study thus far that compared patients who remained on therapeutic warfarin to those who discontinued warfarin for the procedure, the risk of stroke or TIA was significantly lower on warfarin, even after accounting for age, gender, type of AF, and CHADS2 score.(5) Importantly, no significant increase in the incidence of bleeding complications, including cardiac tamponade, has been observed in patients with a therapeutic INR. In fact, several investigators have reported higher rates of groin bruising, discomfort, or frank hematomas in patients off of warfarin, presumably due to the need for post-procedure bridging with unfractionated or low-molecular weight heparin.(2,6,7) Operators need to be aware that less heparin may be necessary to achieve the target ACT in patients who present with an INR greater than 2.0.(6)
Several techniques have been reported to significantly decrease the incidence of peri-procedural stroke or formation of left atrial thrombus during the ablation procedure, including flushing the sheaths with high-dose heparin prior to intravenous access,(8) high-rate sheath perfusion during the procedure, (9) administration of intravenous heparin prior to transseptal puncture rather than afterwards,(10) and maintenance of a higher minimum ACT during the procedure.(11) Despite these precautions, however, thrombus formation is still occasionally observed, with patient risk factors that include the presence of spontaneous echo contrast in the left atrium pre-procedure, larger left atrial size, and persistent atrial fibrillation.(12)
There are no consensus guidelines for the management of catheter-associated and sheath-associated thrombus discovered in the left atrium during ablation procedures, and the relative infrequency of the complication has precluded any comparative trial. In cases during which the ACT was sub-therapeutic at the time of thrombus discovery, most investigators have advocated administration of additional heparin as the initial step in management.(12-15) In the two largest published case series, withdrawal of the catheters and sheaths to the right atrium was effective in removing the thrombus in the majority of patients.(10, 12) Both withdrawal of the catheter and sheath together as a single unit and withdrawal of the catheter into the sheath prior to removal from the left atrium have been reported.(10-13) Several investigators have also simultaneously aspirated the sheaths via the side port during catheter removal, with retrieval of thrombus in many cases.(8, 10, 13, 14) It is reassuring that no thromboembolic complications have been reported is association with attempts at thrombus removal, though that may also be related to some degree of reporting bias.
There have also been case reports of successful thrombus management with lytic therapy,(15) as well as with suction via two transseptal sheaths in parallel, with thrombus retrieval via the sheath without the associated catheter thrombus.(16) Efforts at cerebrovascular protection have also been made with placement of bilateral temporary carotid artery filters or a multielectrode basket catheter in the ascending aorta.(10, 14)
Our patient was maintained on therapeutic warfarin for his procedure and received heparin prior to transseptal puncture with a target ACT >350 secs. However, he did have significant left atrial enlargement, spontaneous echo contrast noted on pre-procedure TEE, and a sub-therapeutic ACT despite appropriate weight-based heparin dosing. The thrombus appeared attached to the circular mapping catheter, as has been frequently reported in these situations, and it did not decrease significantly in size despite subsequent maintenance of ACT >350 for more than 15 minutes. The mapping catheter was withdrawn back to, though not inside, the transseptal sheath. The thrombus was not retrieved by aspiration of the sheath, so the sheath and catheter were pulled back into the right atrium under ICE guidance while simultaneously applying suction to the sideport. The thrombus was successfully removed, and the procedure was completed without further complication. There has been no evidence of any thromboembolic sequelae through 9 months of follow-up.
References
Cappato R, Calkins H, Chen S-A et al. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation 2005;111:1100-5.
Wazni OM, Beheiry S, Fahmy T et al. Atrial fibrillation ablation in patients with therapeutic international normalized ratio:comparison of strategies of anticoagulation management in the periprocedural period. Circulation 2007;116:2531-4
Hussein AA, Martin DO, Saliba W et al. Radiofrequency ablation of atrial fibrillation under therapeutic international normalized ratio:a safe and efficacious periprocedural anticoagulation strategy. Heart Rhythm 2009;6:1425-9.
Schmidt M, Segerson NM, Marschang H et al. Atrial fibrillation ablation in patients with therapeutic international normalized ratios. PACE 2009;32:995-9.
Di Biase L, Burkhardt JD, Mohanty P et al. Periprocedural stroke and management of major bleeding complications in patients undergoing catheter ablation of atrial fibrillation:the impact of periprocedural therapeutic international normalized ratio. Circulation 2010;121:2550-6.
Gautam S, John RM, Stevenson WG et al. Effect of therapeutic INR on activated clotting times, heparin dosage, and bleeding risk during ablation of atrial fibrillation. J Cardiovasc Electrophysiol 2011;22:248-54.
Page SP, Siddiqui MS, Finlay M et al. Catheter ablation for atrial fibrillation on uninterrupted warfarin:can it be done without echo guidance? J Cardiovasc Electrophysiol 2011;22:265-70.
Maleki K, Mohammadi R, Hart D et al. Intracardiac ultrasound detection of thrombus on transseptal sheath:incidence, treatment, and prevention. J Cardiovasc Electrophysiol 2005;16:561-5.
Cauchemez B, Extramiana F, Cauchemez S et al. High-flow perfusion of sheaths for prevention of thromboembolic complications during complex catheter ablation in the left atrium. J Cardiovasc Electrophysiol 2004;15:276-83.
Bruce CJ, Friedman PA, Narayan O et al. Early heparinization decreases the incidence of left atrial thrombi detected by intracardiac echocardiography during radiofrequency ablation for atrial fibrillation. J Interv Card Electrophysiol 2008;22:211-9.
Ren J-F, Marchlinski FE, Callans DC et al. Increased intensity of anticoagulation may reduce risk of thrombus during atrial fibrillation ablation procedures in patients with spontaneous echo contrast. J Cardiovasc Electrophysiol 2005;16:474-7.
Ren J-F, Marchlinski FE, Callans DC. Left atrial thrombus associated with ablation for atrial fibrillation:identification with intracardiac echocardiography. J Am Coll Cardiol 2004;43:1861-7.
Keane D, Mansour M, Singh J. Detection by intracardiac echocardiography of early formation of left atrial thrombus during pulmonary vein isolation. Europace 2004;6:109-110.
Martelo S, D’Avila A, Ferreira F et al. Implantation of bilateral carotid artery filters to allow safe removal of left atrial thrombus during ablation of atrial fibrillation. J Cardiovasc Electrophysiol 2006;17:1140-1.
Okuyama Y, Kashiwase K, Mizuno H et al. Development of thrombus on a transseptal sheath in the left atrium during attempted electrical pulmonary vein isolation for the treatment of paroxysmal atrial fibrillation. Europace 2006;8:191-2.