51-year-old female with hypertrophic cardiomyopathy and a history of recurrent AF for which she began taking amiodarone 200 mg PO daily 18 months ago. Mild hypothyroidism was noted 3 months after starting amiodarone, and a small dose of synthroid was prescribed and amiodarone was continued.
Other pertinent medical history includes sinoatrial node dysfunction for which a dual chamber pacemaker was implanted in 1999.
At her last visit to clinic several months earlier, she had no complaints, and pacemaker interrogation revealed normal device function with minimal atrial fibrillation. She now presents to the hospital emergency department with dyspnea, lower extremity edema and palpitations. In addition she complains of an unintentional 10 pound weight loss and GI irritability over the past month.
Based on the above information, the next best step in evaluation would be:
Show Answer
The correct answer is: C. Additional laboratory evaluation.
Long standing use of amiodarone raises the question of amiodarone-induced thyrotoxicity, despite the history of thyroid suppression earlier in the treatment course. A TSH level revealed the correct diagnosis. A suppressed TSH level and elevated T3 and FT4 values are virtually diagnostic.
Thyroid Labs (provide range of normal) TSH 0.10 mIU/L Free T4 21.5 ng/dl T3 261 ng/dl
Coronary angiography is not the best choice for immediate management because, although there is a mild elevation in cardiac biomarkers, there is not strong evidence of an acute coronary syndrome and her presentation could be explained by atrial arrhythmia with rapid ventricular rates aggravating diastolic dysfunction from underlying hypertrophic cardiomyopathy. Additionally, iodine based contrast sometimes used in diagnostic imaging procedures may worsen hyperthyroidism acutely.(1)
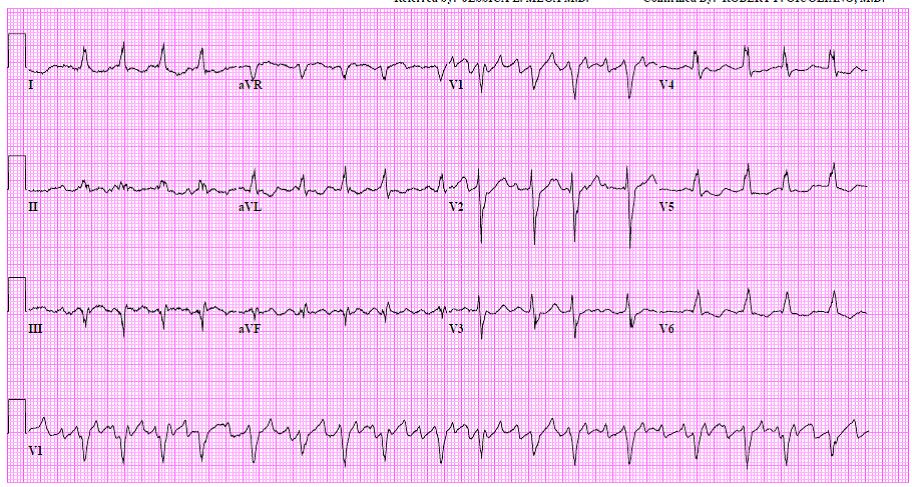
Immediate direct current CV is inappropriate since she is hemodynamically stable and we do not know her recent INR values or the onset of AF. CV in the setting of inadequate anticoagulation and a prolonged AF episode (> 48 hrs) would expose her to significant risk of thromboembolism. Likewise, catheter ablation is a poor choice for rhythm control for the same reasons and the fact that the underlying rhythm is atrial fibrillation, not flutter. Although the rhythm appears to be organized in lead V1, careful inspection of other leads shows more chaotic, irregular activity without a defined P wave morphology, indicating atrial fibrillation.
Amiodarone is an effective anti-arrhythmic drug, but is not labeled for use in atrial fibrillation by the FDA. It can cause severe adverse effects, including thyroid dysfunction; hypothyroidism develops in 6% and thyrotoxicosis in 12% to 15% of patients.(2) Amiodarone-induced thyrotoxicosis is prevalent in populations with low iodine intake, whereas hypothyroidism occurs in people in areas with high iodine intake.(3) Unlike hypothyroidism, which is rare after the first 18 months of therapy, hyperthroidism can occur at any time throughout the duration of treatment. Thyroid toxicity may develop both in apparently normal thyroid glands and in glands with preexisting abnormalities.(3) As in this patient’s case, oral thyroid hormone replacement therapy places patients at higher risk of developing clinically significant hyperthyroidism.(4) Amiodarone can cause excess thyroid hormone synthesis (type I), due to the high iodine content of amiodarone, or destructive thyroiditis (type II). Mixed forms of thyrotoxicosis often occur. The other pathogenic mechanisms include disturbance of thyroid iodine autoregulation and induction of thyroid antibodies.(5)
Initial management strategy of our patient included discontinuation of the offending agent and heart rate control with regular release metoprolol. After consultation with our endocrine colleagues, prednisone and methimazole were administered. Over the course of two weeks, the thyroid indices normalized, and her AF was treated with rate control and anticoagulation with future consideration of alternative antiarrhythmic medications and/or catheter ablation. If it were necessary to continue amiodarone, one could have considered chemical or surgical thyroidectomy or chronic suppression with methimazole.(6-7)
References
Fradkin JE, Wolff J. Iodide-induced thyrotoxicosis. Medicine. 1983; 62:1.
Trip MD, Wiersinga W, Plomp TA: Incidence, predictability and pathogenesis of amiodarone-induced thyrotoxicosis and hypothyroidism. Am J Med. 1991; 91:507-511
Batcher EL, Tang XC, Singh BN, et al. Thyroid function abnormalities during amiodarone therapy for persistent atrial fibrillation. Am J Med. 2007; 120:880.
Uzan L, Guignat L, Meune C, et al. Continuation of amiodarone therapy despite type II amiodarone-induced thyrotoxicosis. Drug Saf. 2006; 29:231.
Houghton SG, Farley DR, Brennan MD, et al. Surgical management of amiodarone-associated thyrotoxicosis: Mayo Clinic experience. World J Surg. 2004; 28:1083.
Farwell AP, Abend SL, Huang SK, et al. Thyroidectomy for amiodarone-induced thyrotoxicosis. JAMA. 1990; 263:1526.