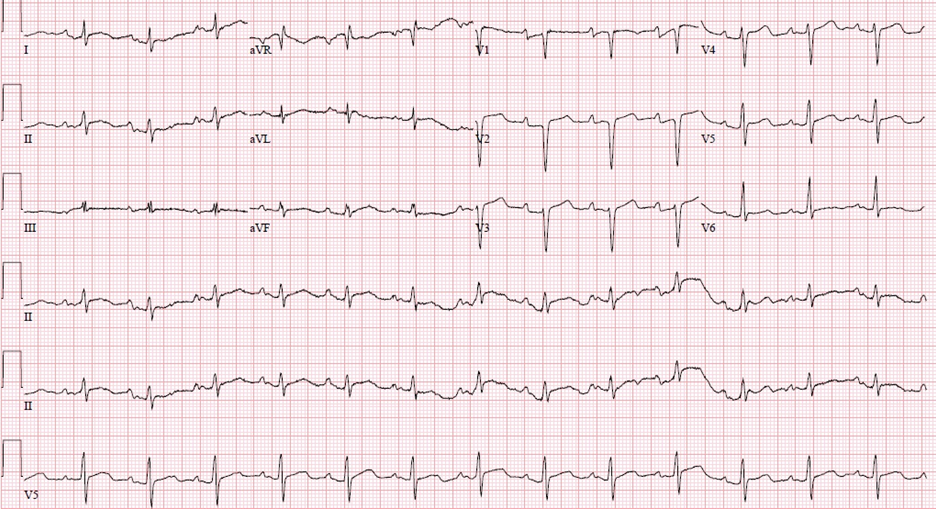
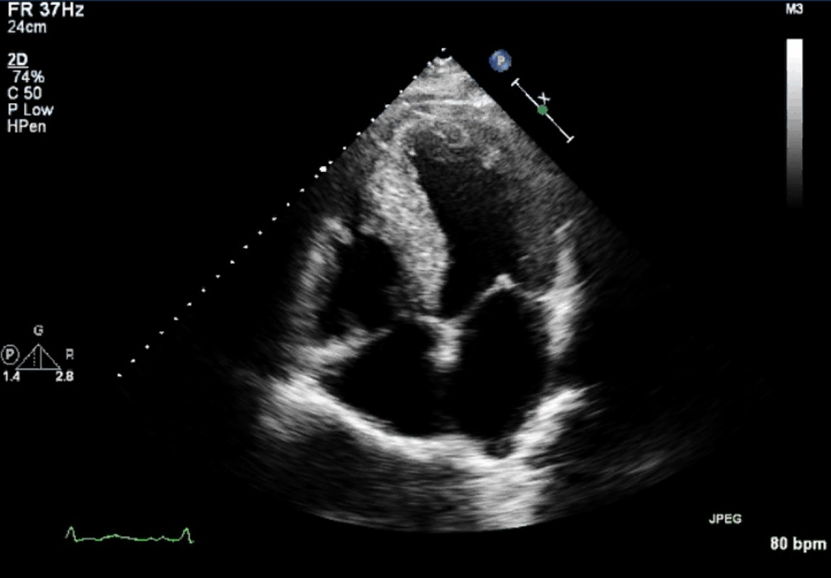
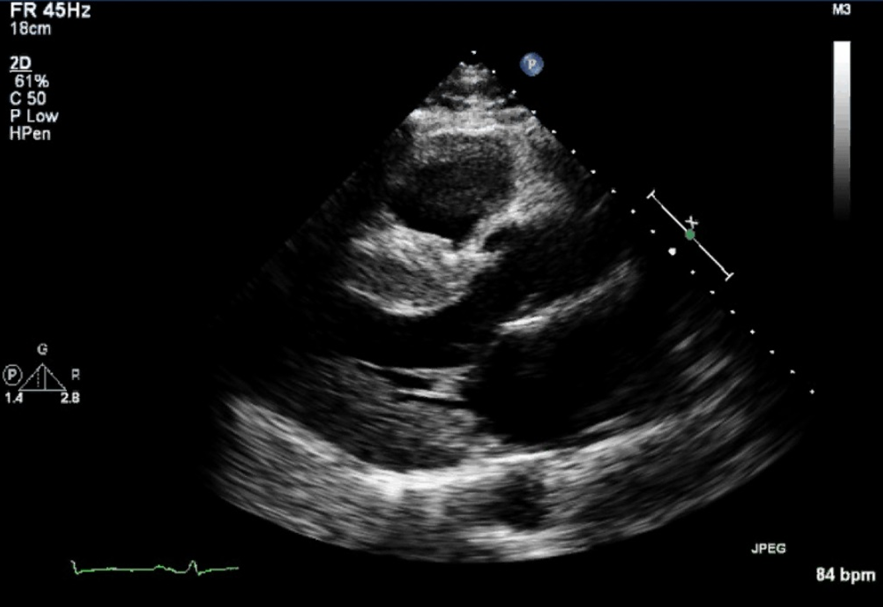
A 53-year-old man with history of hypertension presents with gradually worsening shortness of breath and atypical chest pain for a few months. He is a retired professional football player. Symptoms are associated with orthopnea and paroxysmal nocturnal dyspnea; HIV, antinuclear antibody, creatinine, ceruloplasmin, ferritin, angiotensin-converting enzyme, thyroid stimulating hormone and serum protein electrophoresis were normal. Electrocardiogram demonstrates normal sinus rhythm with low voltage and first degree atrioventricular block. His physical examination is consistent with acute decompensated heart failure. Echocardiogram reveals increased thickening of left ventricular wall (end diastolic inter-ventricular septum diameter of 13 mm), with mildly reduced left ventricular systolic function (estimated left ventricular ejection fraction of 40-45%), and left atrial enlargement (see Figures 1, 2 and 3). Cardiac catheterization demonstrates minimal coronary disease. Cardiac magnetic resonance imaging (MRI) reveals diffuse thickening of left ventricular wall from base to mid cavity. There is global hypokinesis of the left and right ventricles. Both atria are enlarged. There are no perfusion abnormalities, but patchy diffuse heterogeneous late gadolinium enhancement of left ventricular wall, with intramural and subendocardial component from base to apex, and right ventricular inferior wall involvement are present.
Figure 1
Figure 2
Figure 3
Given the above, which of the following describes the most likely diagnosis?
Show Answer
The correct answer is: C. Infiltrative cardiomyopathy
These findings are consistent with an infiltrative non-ischemic cardiomyopathy, and require further evaluation. The delayed myocardial enhancement is not consistent with athlete's heart. The thickness of the walls is not consistent with hypertrophic cardiomyopathy nor hypertension induced cardiomyopathy. The degree of late gadolinium myocardial enhancement and biventricular involvement are also suggestive of an infiltrative process. Cardiac catheterization does not reveal significant coronary artery disease. When evaluating athletes with symptoms, a broad differential is most important, especially in the older athlete or prior athlete.
Endomyocardial biopsy reveale amyloid deposits on Congo red stain. Liquid chromatography tandem mass spectrometry (LC MS/MS) detects a peptide profile consistent with transthyretin amyloidosis (ATTR) (transthyretin/prealbumin)-type amyloid deposition. The above supports the diagnosis of amyloidosis and indicated hereditary ATTR-type amyloid deposition (VAll22I1e). Transthyretin gene sequencing reveals Val122Ile missense mutation in TTR gene (genomic DNA was polymerase chain reaction (PCR)-amplified for exons 1-4 of TTR). The patient is started on carvedilol 12.5 mg per Os (PO) twice per day, olmesartan 40 mg PO daily, and furosemide 40 mg PO daily. His symptoms of shortness of breath improve. He is also placed on list for combined liver and heart transplant.
In amyloid patients with known mutations that are associated with cardiomyopathy, liver transplantation prior to development of cardiac dysfunction can potentially avoid this complication. However, in patients who have already developed significant cardiomyopathy, wild-type amyloid can continue to deposit, negating the benefit of the liver transplantation. Combined heart and liver transplants should be considered in these patients.
References
Schwartz BG, Kuiper JJ, Klintmalm GB, Stone MJ, Schussler JM. Combined cardiac and liver transplantation for the treatment of familial amyloidosis. Proc (Bay Univ Med Cent). 2007;20:146-8.
Topilsky Y, Pereira NL, Shah DK, et al. Left Ventricular assist device therapy in patients with restrictive and hypertrophic cardiomyopathy. Circ Heart Fail. 2011;4:266-75.
AndoY, Coelho T , Berk JL, et al. Guideline of transthyretin-related hereditary amyloidosis for clinicians. Orphanet J of Rare Dis. 2013;8:31.