56-year-old healthy female presents to the emergency department with palpitations associated with lightheadedness and chest discomfort. She has a 20-year history of Wolf-Parkinson White syndrome (WPW) and intermittent palpitations associated with lightheadedness, typically lasting 3-4 minutes. However, she sought medical attention because this particular episode persisted for over an hour. She has never had syncope. She also recently underwent exercise stress testing with nuclear imaging revealing no evidence of ischemia.
Medications: multivitamin, vitamin D, vitamin B12, iron, aspirin 81mg, and fish oil.
Physical examination notable for blood pressure of 151/73 and pulse rate of ~200bpm.
Laboratory Data
WBC 8.3 K/ul, Hct 43.8 %, platelets 327,000 K/ul
Glucose 136 mg/dl
BUN 14 mg/ul
Creatinine 1.0 mg/dl,
Na+ 139 mmol/L
K+ 3.4 mmol/L
CK/CK-MB/troponin T all within normal range.
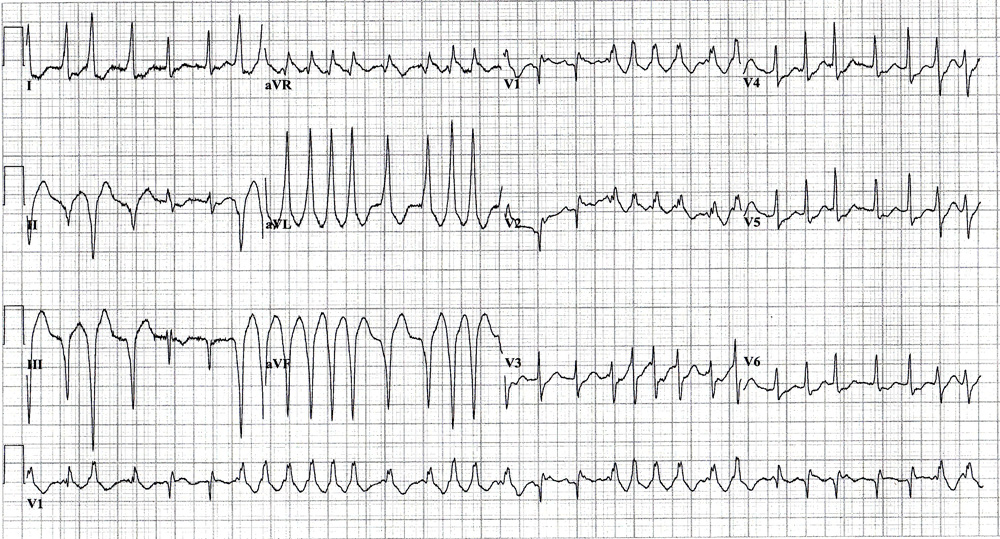
Her presenting electrocardiogram is shown.
Based on the history and electrocardiogram, the most appropriate initial treatment would be:
Show Answer
The correct answer is: C. IV Procainamide
The above electrocardiogram of an irregular wide complex tachycardia shows pre-excited atrial fibrillation in the setting of WPW. This patient actually has a longstanding history of known WPW managed conservatively, but no history of atrial fibrillation. Her prior self-limited episodes of tachycardia were likely due to atrioventricular reciprocating tachycardia (AVRT) utilizing an accessory atrioventricular pathway.
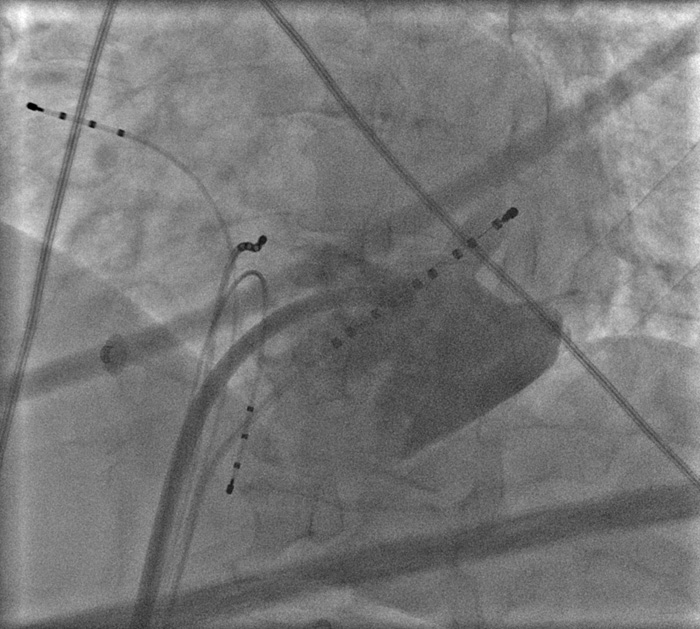
Above: Left Anterior Oblique View
Above: Right Anterior Oblique View
After the above diagnosis was made in the emergency department, the patient was given a bolus of intravenous amiodarone, which is also an effective and safe pharmacologic treatment, however procainamide is considered first line therapy. The mechanism of action is sodium channel blockade, which prolongs anterograde conduction and the refactory period of an accessory pathway, thus slowing the ventricular response. Unfortunately, the patient did not respond to amiodarone and became hemodynamically unstable with symptoms of severe lightheadedness. Therefore, she was given another bolus of amiodarone and cardioverted after being sedated with fentanyl and midazolam. After two attempts, atrial fibrillation converted to normal sinus rhythm. The following day she underwent successful catheter ablation of a posteroseptal accessory pathway from within the neck of a large coronary sinus diverticulum. (See images).
IV diltiazem and adenosine, answers (A) and (B), are incorrect because administration of AV nodal blocking agents in this setting may have deleterious consequences, despite adenosine's very short half-life. By slowing conduction through the AV node, increased anterograde conduction over the accessory pathway may occur as fewer wavefronts are available to render the accessory pathway partially refractory via retrograde penetration. In this way, AV nodal blocking agents may potentially induce ventricular fibrillation. Lidocaine, answer (D), does not significantly affect atrial, AV nodal, or accessory pathway tissue, but could be given inappropriately if the arrhythmia is mistaken for ventricular tachycardia. Cardioversion, answer (E), was ultimately required because of hemodynamic deterioration, however since this patient was initially hemodynamically stable, pharmacologic treatment is recommended first and may help to prevent arrhythmia recurrence following cardioversion.
Discussion
Atrial fibrillation is the most common cardiac arrhythmia encountered in clinical medicine.(1) It can be anticipated that the incidence of AF will continue to rise in the decades to come. Patients with WPW syndrome have a slightly higher risk of sudden cardiac death (0.05 – 0.5% per year) than the general population due to atrial fibrillation inducing ventricular fibrillation.(2) For reasons not entirely known, patients with WPW appear to have an increased likelihood of developing AF, probably due to AVRT leading to AF. It is crucial to appropriately diagnose patients presenting with pre-excited atrial fibrillation because of the potential deleterious outcome when managed inappropriately. More importantly, one should identify individuals with symptomatic WPW to allow for proper risk stratification and treatment as primary prevention. This particular patient's EKG demonstrates high risk features, specifically an R-R interval of less than 200ms.(3) Currently, most patients with symptomatic WPW syndrome are referred for catheter ablation, which is a Class 1 indication.(3) Catheter ablation is both highly successful and safe. In a study of over 6,000 patients undergoing accessory pathway ablations from 1997 – 2002 at several institutions, the long term success rate was 98% and the major complications rate was only 0.6%.(4) One could argue that this patient should have undergone electrophysiologic evaluation and ablation prior to this presentation given her history of recurrent tachycardia and manifest pre-excitation on surface EKG.
References
Wolf PA, Benjamin EJ, Belanger AJ, et al: Secular trends in the prevalence of atrial fibrillation: The Framingham Study. Am Heart J. 1996;131:790-795.
Hogenhuis W, Stevens SK, Wang P, et al. Cost-effectiveness of radiofrequency ablation compared with other strategies in Wolff–Parkinson–White syndrome. Circulation. 1993; 88:II437–46.
Blomstrom-Lundqvist C, Scheinman MM, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias - executive summary.J Am Coll Cardiol. 2003; 42:1493-1531.
Morady F. Catheter ablation of supraventricular arrhythmias: state of the art. J Cardiovasc Electrophysiol. 2004;15:124–39.