A 63-year-old male was transferred to our institution with the chief complaint of palpitations and dizziness for several weeks. His extensive medical history included insulin-dependent diabetes mellitus, hypertension, severe peripheral arterial disease status post right below-knee amputation, and prior ischemic cerebral vascular accident with residual hemiparesis. Preceding the below-knee amputation, which was 2 months prior to current hospitalization, he underwent ischemic evaluation via a pharmacological nuclear (thallium) single-photon emission computed tomography (SPECT) with rest and stress imaging interpreted as transmural apical myocardial infarction (MI) with a small component of inducible ischemia involving the septum. The ejection fraction (EF) was calculated at 32%. A cardiac catheterization was not performed. The patient was assumed to have an ischemic cardiomyopathy by the referring physicians, and guideline-directed medical therapy was initiated.
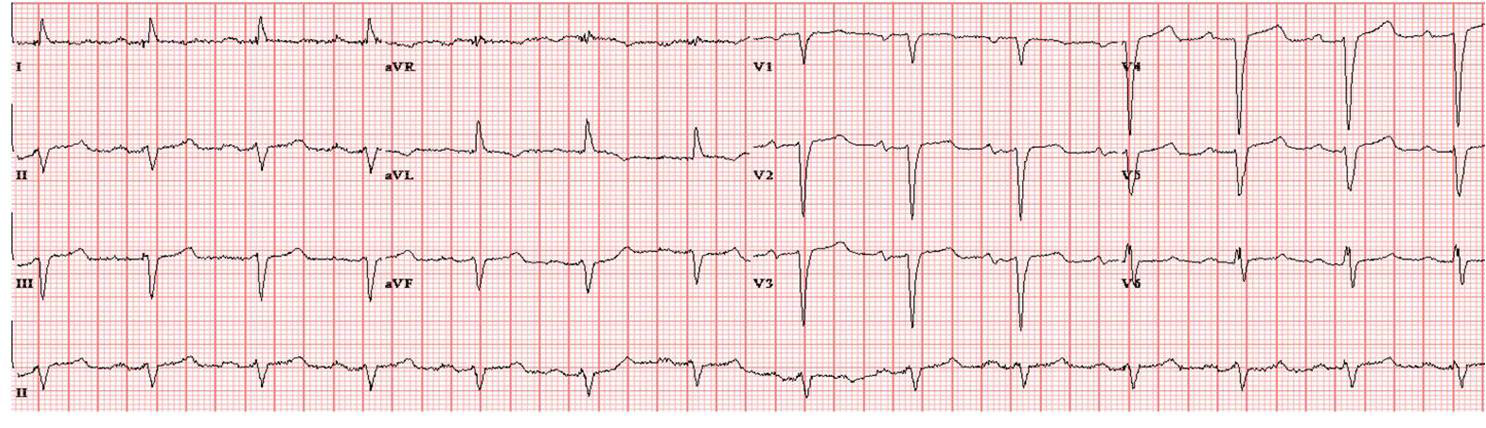
Upon admission at our institution, he denied angina or recent heart failure symptoms. He underwent transthoracic echocardiography that revealed an EF of 25-30% with severe global left ventricular (LV) hypokinesis and, most significantly, anteroseptal and apical akinesis. An electrocardiogram (ECG) showed sinus rhythm with evidence of previous anterior MI (Figure 1). Troponin I was 0.038 (99th percentile upper limit of normal 0.045) with a creatine of 1.06 mg/dl and a glomerular filtration rate >60 mL/min/1.73m2. Given his severe LV dysfunction, electrophysiology consultation was obtained for consideration of an implantable cardioverter defibrillator (ICD). Cardiac catheterization was requested to solidify an etiology of ischemic cardiomyopathy, and the patient underwent diagnostic coronary angiography (Figure 2 and Video 1).
Figure 1. Baseline 12-lead ECG
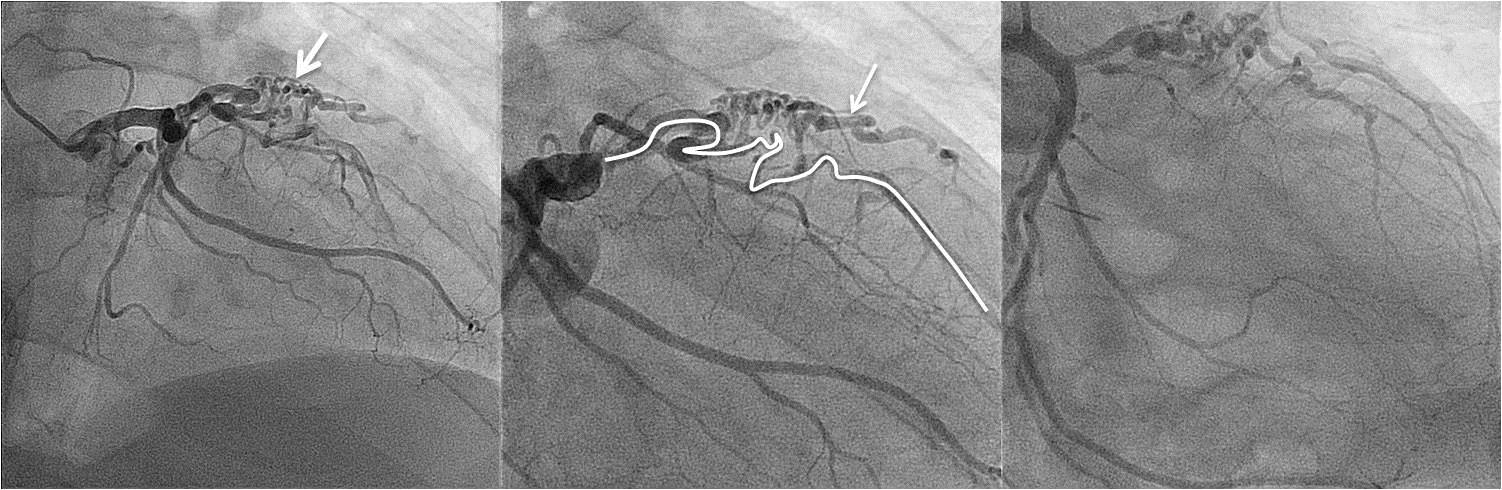
Figure 2. Serial angiographic images illustrating (left) the typical "nest" of tortuous vasculature associated with coronary to pulmonary artery fistulae (white arrow), (middle) the course of the left anterior descending (LAD) artery (white outline) with the diagonal marked (white arrow), and (right) right anterior oblique (RAO) caudal view providing additional fistula visualization.
Video 1. RAO cranial angiography revealing delayed angiographic filling of the distal LAD, likely a result of both multiple fistulous vessels and some degree of concomitant coronary artery disease. Note the absence of the typical dilated feeder vessels or distal connection to the pulmonary artery as a result of spontaneous closure.
Given this patient's presenting symptoms and angiographic findings, was would the most likely diagnosis and next step in clinical management include?
Show Answer
The correct answer is: D. Findings represent a coronary artery to pulmonary artery fistula with thrombotic, spontaneous closure of the distal connection. No additional imaging or therapy, specifically fistula closure, is warranted given the current clinical and angiographic findings. Proceed with ICD consideration.
A full discussion of the typical appearance, etiology, and indications for closure follows.
Vascular communications between coronary arteries and other vessels (coronary artery arteriovenous malformations) or cardiac chambers (coronary-cameral fistulae) are rare in adulthood, with an incidence ranging from 0.3-0.8% at time of angiography.1 That said, experienced interventionalists will undoubtedly encounter this anomaly at some point during their training and should understand the anatomy, pathophysiological, and management options.
Coronary arterial-venous fistulae typically are the result of deviations during normal embryological development. However, they can also be acquired after penetrating chest wall trauma or following cardiac procedures such as endomyocardial biopsy, pacemaker implantation, or even coronary angiography, none of which played a role in the presented case. The most common site of origin is the right coronary artery (55%) followed by the left coronary artery system (35%), with duel coronary systems compromising only 5%.1 They are also commonly found in patients with chronic systemic arterial desaturation, especially in the setting of adults with longstanding treated forms of cyanotic congenital heart disease (especially single ventricles). In our case, the pulmonary arteries served as the termination site, although this is only the case in a minority of situations (17%). For the most part, these vascular communications terminate in the right ventricle (40%) or the right atrium (26%). Coronary artery fistulae can also rarely drain to another vascular structure, and the coronary sinus is the most common site for a direct vascular connection.
Angiographically, these anomalies often have a dilated feeder vessel with an abnormal, swirling flow pattern identified. It is important to understand that the feeder vessel is always a normal branch of the coronary artery system. Importantly, when the fistulae are connected to a lower resistance chamber or vessel that allows large amounts of "run-off" blood flow, the more proximal feeder vessel becomes quite dilated. This dilation of the proximal feeder coronary artery branch constitutes one of the key hallmarks for the substrate of run-off "steal" from the intended myocardial blood flow destination. When this is seen, strong consideration for closure should be made to avoid possible supply-demand mismatch during periods of increased myocardial blood flow demand. Extreme vessel tortuosity and a "nest" of network collaterals are usually present and pathopneumonic for coronary artery fistulae. The number of tortuous vessels is less important and not an indication for treatment; however, the caliber of the point of where the fistula drains can be sizeable and is important with respect to the risk for myocardial blood flow steal. In certain cases, anastomoses or collateral networks are small and not well visualized. This makes obstructive lesions difficult to assess, as demonstrated in this case with spontaneous closure and no further high-flow shunt physiology that produces the typical dilated feeder vessel. Only a nest of small, tortuous coronary vasculature remains.
The majority of coronary arterial-venous fistulae are small and thus asymptomatic, only to be discovered at a time of coronary angiography. Large, hemodynamically significant coronary arterial-venous fistulae are typically three times the size of a normal caliber coronary artery producing ischemia via a coronary steal phenomena, volume overload, and heart failure as a result of left to right shunting, fistula rupture or thrombosis, arrhythmias, and even endocarditis.2
It is the recommendation of the American College of Cardiology and American Heart Association to close all large coronary artery fistulae, irrespective of symptomatology, by way of surgical or transcatheter techniques. Small-to-moderate fistulae warrant treatment only when symptomatic.3 Historically, surgical closure has been considered the primary treatment modality. However, percutaneous methods utilizing percutaneous vascular occluder devices or coil embolization are viable options in select patients.4, 5
The current case presents somewhat of a challenge regarding the clinical management. There is suspected concomitant coronary artery disease at the level of the fistula, although it is not clear if the vessel narrowing is entirely related to atherosclerotic disease or native vessel fistula involvement. Spontaneous fistula thrombosis with subsequent closure has been reported in both the pediatric and adult populations.6-8 Management strategies in these cases require individualization but can generally be guided with the same criteria as the guidelines suggest. In many cases, particularly where the fistula enters through the wall of the pulmonary artery, the fistulae will become closed by the gradual buildup of fibro-intimal tissue, thus severely restricting or even completely shutting off the flow through the fistula. In a series of 31 asymptomatic patients with echocardiographic and/or angiographic findings of coronary arterial-venous fistulae, no patient reported symptoms after more than 2 years of follow-up.9 In fact, spontaneous closure occurred in 23% of patients, further suggesting the role of a "watch and wait" strategy for clinically silent coronary fistulae.
In the current case, one could argue to pursue closure of the proximal fistula anastomosis in hopes of salvaging some LV function. However, both the nuclear SPECT and ECG suggesting transmural infarct, along with the absence of ongoing ischemic or heart failure symptoms, strongly suggested that the fistula was not the etiology; therefore, closure was not pursued. Additionally, intervention at this juncture is unlikely to improve the severe, global LV dysfunction. It is unlikely any intervention to the fistula even if it were open would change LV function particularly because the patient had no angina as a reason for ischemic therapy. In addition, the fistula may be partially and separately supplying the LV myocardium, and its closure without a communication could create additional anterior ischemia or, at worst, infarction. The typical dilation of the coronary vasculature was not seen in this case as a result of thrombosis, which is a finding that should raise suspicion of spontaneous distal closure.
In summary, coronary arterial-venous fistulae are an uncommon finding at the time of angiography with spontaneous restriction or closure possible. The extreme vessel tortuosity and nest of collaterals angiographically is pathopneumonic for coronary fistulous formation, either to another vessel (coronary artery arteriovenous malformations) or cardiac chamber (coronary-cameral fistulae). Consideration for closure is currently indicated for large and/or hemodynamically significant coronary arterial-venous fistulae, or when symptoms are felt attributable to this fistulous communication. Improvement in devices and techniques now allows for transcatheter closure of many coronary arterial-venous fistulae in experienced hands. In the instance of spontaneous closure with continued fistulous remnants, treatment should also be guideline directed. The data to support this are by case series only, and ultimately the clinician's judgment and individualized therapy are required.
Editor's Note: This Patient Case Quiz has stumped even our reviewers! I was unsure myself and asked for review help from two senior interventional colleagues, one of whom is an adult congenital expert. Given the images available, there is debate as to whether this is a congenital aneurism/fistula or a chronic LAD occlusion/aneurism with collaterals. One even wonders if remote chest trauma could be a contributor to a chronic LAD occlusion with aneurism collateral circulation as an alternate explanation.
It's a great case that makes us all think, and from that standpoint alone it makes a good exercise.
From George W. Vetrovec, MD, MACC
References
Gowda RM, Vasavada BC, Khan IA. Coronary artery fistulas: clinical and therapeutic considerations. Int J Cardiol 2006;107:7-10.
Tirilomis T, Aleksic I, Busch T, Zenker D, Ruschewski W, Dalichau H. Congenital coronary artery fistulas in adults: surgical treatment and outcome. Int J Cardiol 2005;98:57-9.
Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease). Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2008;52:e143-263.
Armsby LR, Keane JF, Sherwood MC, Forbess JM, Perry SB, Lock JE. Management of coronary artery fistulae. Patient selection and results of transcatheter closure. J Am Coll Cardiol 2002;39:1026-32.
Jama A, Barsoum M, Bjarnason H, Holmes DR Jr, Rihal CS. Percutaneous closure of congenital coronary artery fistulae: results and angiographic follow-up. JACC Cardiovasc Interv 2011;4:814-21.
Sapin P, Frantz E, Jain A, Nichols TC, Dehmer GJ. Coronary artery fistula: an abnormality affecting all age groups. Medicine (Baltimore) 1990;69:101-13.
Hackett D, Hallidie-Smith KA. Spontaneous closure of coronary artery fistula. Br Heart J 1984;52:477-9.
Schleich JM, Rey C, Gewillig M, Bozio A. Spontaneous closure of congenital coronary artery fistulas. Heart 2001;85:E6.
Sherwood MC, Rockenmacher S, Colan SD, Geva T. Prognostic significance of clinically silent coronary artery fistulas. Am J Cardiol 1999;83:407-11.