Thank you for visiting ACC.org. Please note that this item was published more than 5 years ago and therefore its content may be outdated. For more current information on this topic, we encourage you to visit our Congenital Heart Disease and Pediatric Cardiology Collection page.
A 6-year-old girl presents to the emergency room with recurrent shortness of breath and cough. She has a history of poorly controlled, moderately persistent bronchial asthma that has required multiple pediatric intensive care unit admissions due to recurrent pneumonia and status asthmatics, despite good compliance to asthma medications.
Review of systems reveals no history of chest pain, fatigue, dizziness, syncope hemoptysis, weight loss, trauma, vomiting, or diarrhea. There is no history of contact with sick patients, recent travel, or family history of immunodeficiency, sudden death, or congenital heart disease.
On physical examination, she has no dysmorphic features, with appropriate growth parameters for age and gender. Her respiratory rate is 26/minute, and room air oxygen saturation is 99%. Lung exam reveals decreased breath sounds in the right lower lobe. Cardiovascular examination reveals a point of maximum intensity at the right 5th intercostal space mid-axillary line. The remainder of the exam is normal.
Routine laboratory analysis, including a complete blood count and metabolic panel, is normal. A postero-anterior chest roentgenogram is shown in Figure 1. Chest computed tomography (CT) without IV contrast (Figure 2), and gadolinium enhanced magnetic resonance angiogram (Figures 3 and 4) are also obtained. A decision is made to perform a cardiac catheterization (Figures 5 and 6) for further evaluation.
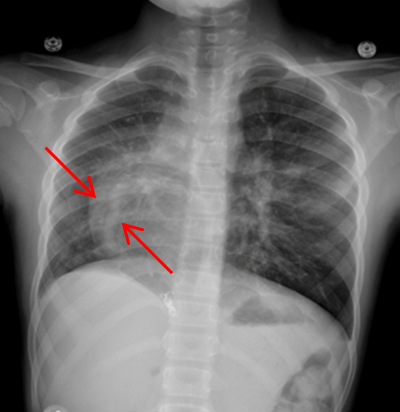
Figure 1
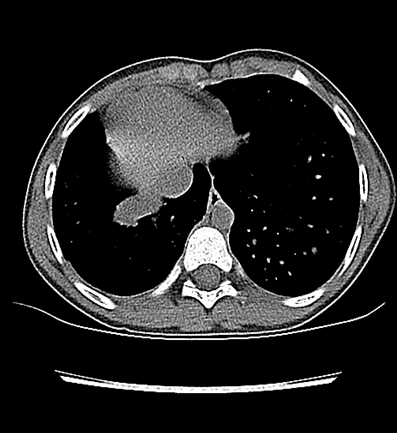
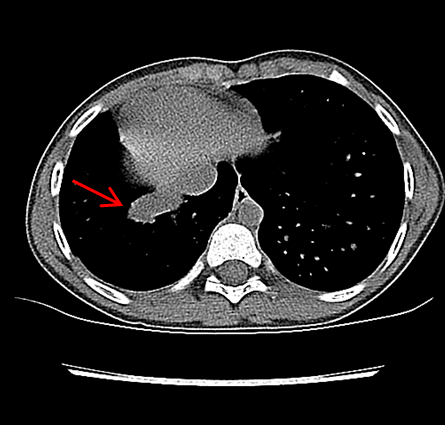
Figure 2
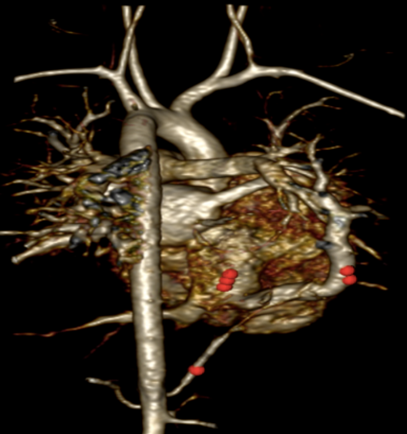
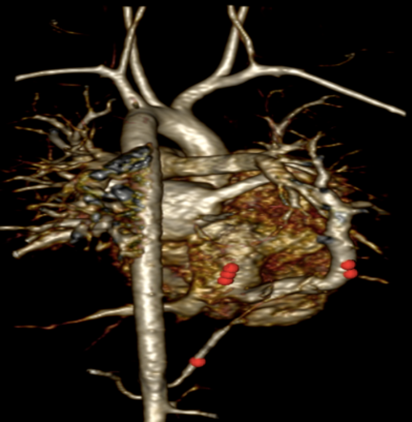
Figure 3
Figure 4
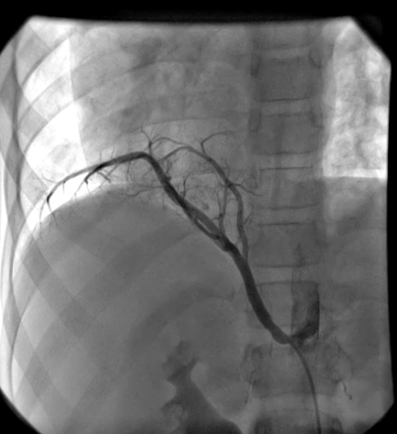
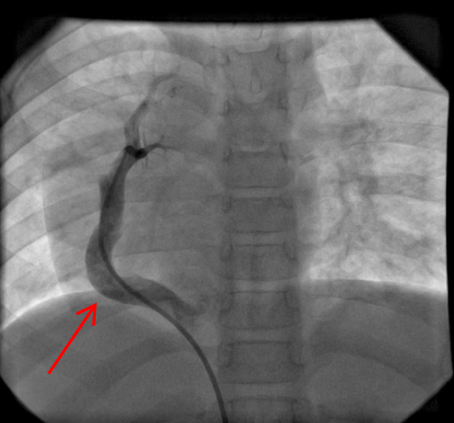
Figure 5
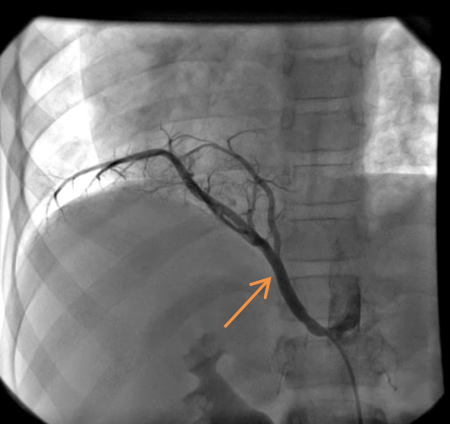
Figure 6
Which of the following describes the most likely diagnosis?
Show Answer
The correct answer is: B. Scimitar syndrome.
This patient is diagnosed with scimitar syndrome associated with secondary dextro-position of the heart due to lower lobe hypoplasia of the right lung and associated sequestration. An anomalous systemic arterial connection between the descending aorta and the right lower lobe is also found.
Scimitar syndrome or congenital venolobar syndrome is a rare congenital heart disease characterized by drainage of partial anomalous pulmonary veins of the right lung (often middle and lower lobes) into the inferior vena cava (IVC). This makes a crescent-shaped shadow parallel to the right heart border, likened to the scimitar sword, on chest roentgenography (Figure 7). Patients with scimitar syndrome also have some hypoplasia of the right lung with associated dextro-position of the heart. Aortopulmonary collateral vessels and atrial septal defects are also commonly seen in patients with Scimitar syndrome in addition to extracardiac anomalies.1,2,3
The red arrow (Figures 7, 8, 9, and 11) shows a large scimitar vein. Chest CT (Figure 8) shows partial anomalous pulmonary venous return from the right lower pulmonary vein into the inferior vena cava (IVC) and right-sided pulmonary hypoplasia with consequent dextro-position of the heart into the right hemithorax. The gadolinium-enhanced angiography cardiac magnetic resonance imaging (MRI) (Figure 9) with three-dimensional reconstruction (Figure 10, Video 1) confirms the diagnosis, which shows aortopulmonary collaterals from the descending abdominal aorta to the right lower lung lobe (one dot), large anomalous pulmonary vein, the scimitar vein (two dots), draining the right lower lung to the IVC (three dots). The right heart is within normal limits for size.
A cardiac catheterization is performed. Right pulmonary artery and descending aorta injections (Figures 11 and 12) show a large scimitar vein and aortopulmonary collaterals to the right lung (orange arrow, Video 2). Coil occlusion of the aortopulmonary collateral is done at the time of the cardiac catheterization. Qp:Qs was 1.3:1 on both MRI and on cardiac catheterization.
As the patient does not have right heart enlargement, the anomalous pulmonary venous connection is not surgically repaired. Following coil occlusion, the patient's symptoms improve dramatically.
This patient has no dysmorphic features, normal liver function, and normal electrolytes which make answer option C (alagille syndrome) an unlikely diagnoses. Dextro-position is secondary to right lung hypoplasia and is not an isolated finding (answer option A). Peripheral pulmonary stenosis (answer option D) would not explain the findings on physical examination and radiological imaging. The patient has been compliant with aggressive asthma management with no improvement making option E less likely.