An 84-year-old man with a history of coronary artery disease status post remote coronary artery bypass graft surgery, carotid artery stenosis status post carotid endarterectomy, hypertension, dysplipidemia, temporal arteritis, squamous cell carcinoma of the skin, benign prostatic hypertrophy, renal insufficiency, multinodular goiter, and osteoarthritis status post total knee arthroplasty presented with progressive dyspnea on exertion. Physical examination was notable for a regular rhythm with a harsh, III/VI mid-late-peaking systolic murmur at the base with preserved S2, as well as 1+ carotid pulses with a faint left carotid bruit. The Society for Thoracic Surgeons (STS) risk calculator predicted a mortality risk for aortic valve replacement of 5.9%, and the patient also met 2 frailty metrics (i.e., walker dependence with impaired 5 meter walk time and reduced grip strength).
Transthoracic echocardiography was notable for a calcified aortic valve with mean gradient of 34 mmHg, aortic valve area (AVA) of 1.1 cm2 with indexed AVA 0.5 cm2/m2, and ejection fraction of 54% without other significant abnormalities (Figure 1). Cardiac catheterization revealed patent bypass grafts and severely diseased native circulation, with a mean aortic valve gradient of 44 mmHg. Computed tomographic angiography (CTA) was notable for a large aortic annulus measuring 33 x 24 mm with calculated circumference 89 mm and area 5.8 cm2, as well as highly calcified ileofemoral vessels with minimal common femoral artery diameters of 4-5 mm (Figure 2). It is of note that because of renal insufficiency, a low-dose contrast protocol was used, raising concern regarding the accuracy of the annular measurements.
Figure 1 (Video)
Figure 2 (Image)
What is the best next step?
Show Answer
The correct answer is: D. Additional imaging
Though the patient's STS risk is in the intermediate range (4-8%), he meets two frailty metrics and is walker dependent. Given the presence of severe symptomatic aortic stenosis (AS), both SAVR and TAVR are reasonable considerations. In this case, the heart team recommended TAVR. However, both the patient's large aortic annulus and borderline femoral access were of some concern.
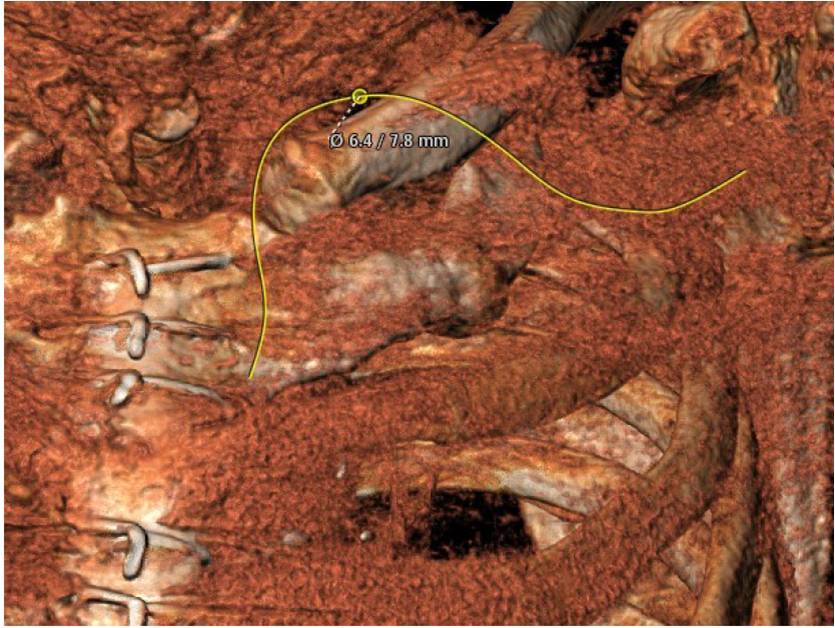
First, the CTA was reviewed for additional dedicated evaluation of the subclavian arteries. This review disclosed a minimum left subclavian artery diameter of 6.4 x 7.8 mm (Figure 3), suggesting the subclavian approach as an attractive point of access.
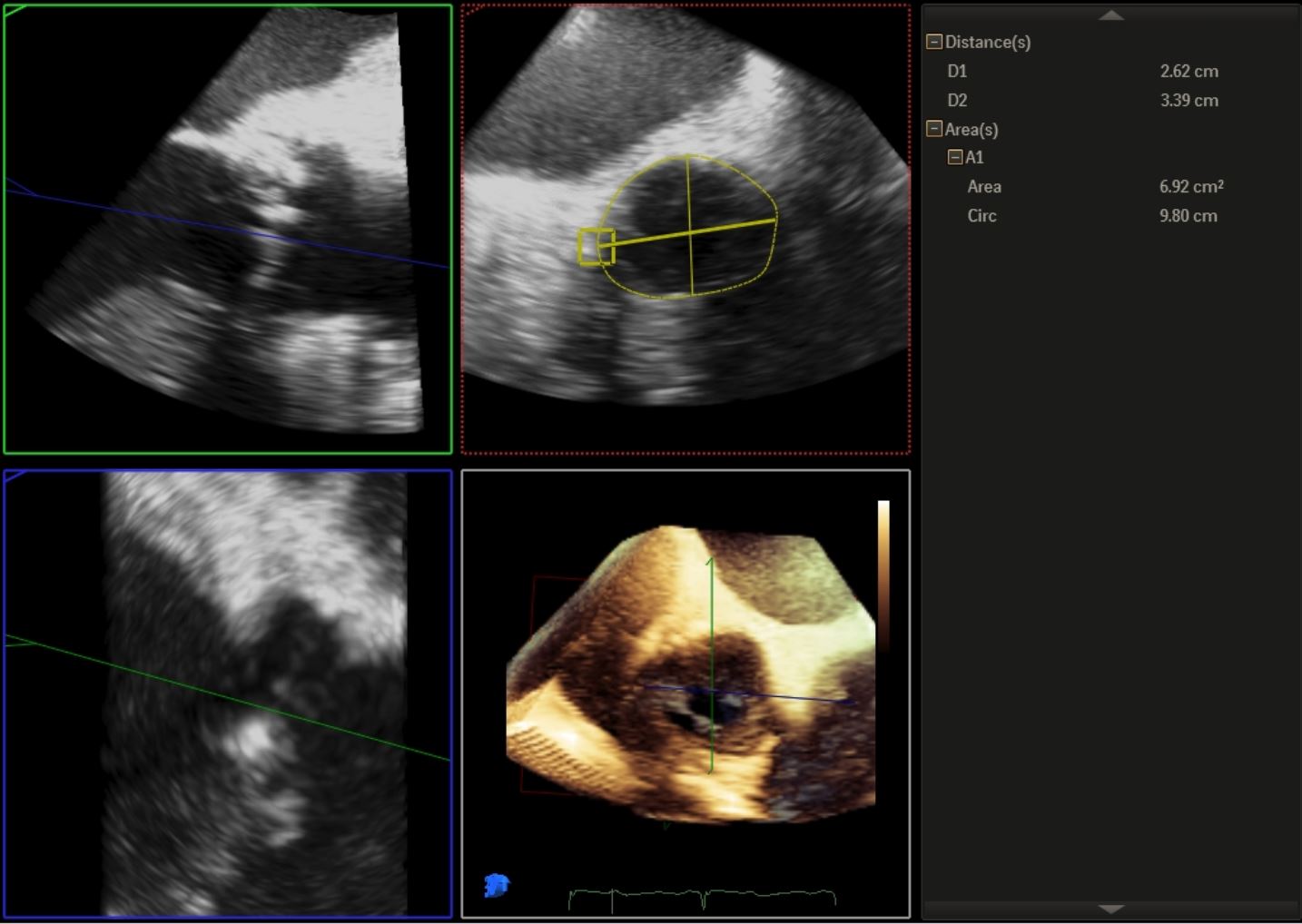
We also referred the patient for transesophageal echocardiography (TEE) with 3-dimensional reconstructions (Figure 4). This study confirmed the presence of severe AS with an estimated annular area of 690 mm2 and perimeter of 98 mm.
The maximal recommended annular circumference for one type of device made by Medtronic is 91.1 mm, and the maximal area for another type of device made by Edwards is 680 cm2 (based on manufacturer data). However, in our experience, it has proven possible to safely deploy the latter system in carefully selected patients with an annulus slightly above the upper limit.
Although CTA has become the standard imaging modality for pre-TAVR planning, TEE may provide substantial complementary data, particularly in cases in which annular dimensions or other aspects of the imaging may be in question.1 In this case, the TEE imaging provided critical additional information, suggesting a circumference that ruled out the use of the Medtronic device.
Taking these data into consideration, the heart team ultimately decided in favor of TAVR via the left subclavian approach. This was performed via surgical cutdown and temporary anastomosis of an 8 mm Dacron chimney graft to the left subclavian artery (Figure 5). The TAVR delivery sheath was inserted into the graft to facilitate hemostasis, and successful balloon valvuloplasty and valve deployment were performed (Figure 6). The transcatheter valve was well seated with no paravalvular regurgitation. The patient had an uncomplicated subsequent course and reported significant symptomatic improvement at his 3-month follow-up.
Figure 3 (Image)
Figure 4 (Image)
Figure 5 (Video)
Figure 6 (Video)
References
Jilaihawa H, Doctor N, Kashif M, et al. Aortic annular sizing for transcatheter aortic valve replacement using cross-sectional 3-dimensional transesophageal echocardiography. J Am Coll Cardiol 2013;61:908-16.