A 17-Year-Old Soccer Player With Mosaic Turner Syndrome on Growth Hormone With a Bicuspid Aortic Valve, Mild AS, and Aortic Dilation
A 16–year-old female with mosaic Turner syndrome (TS) on growth hormone (GH) therapy has a history of a bicuspid aortic valve and mild aortic stenosis (AS). She presents for her annual cardiac clearance for sports participation. She has been followed for several years with trending of her aortic measurements and aortic valve gradient. She is a competitive soccer player and plays on several travel teams. She plans to play competitively in college. She is otherwise healthy and feels well. She is followed by cardiology and endocrinology regularly.
|
|||
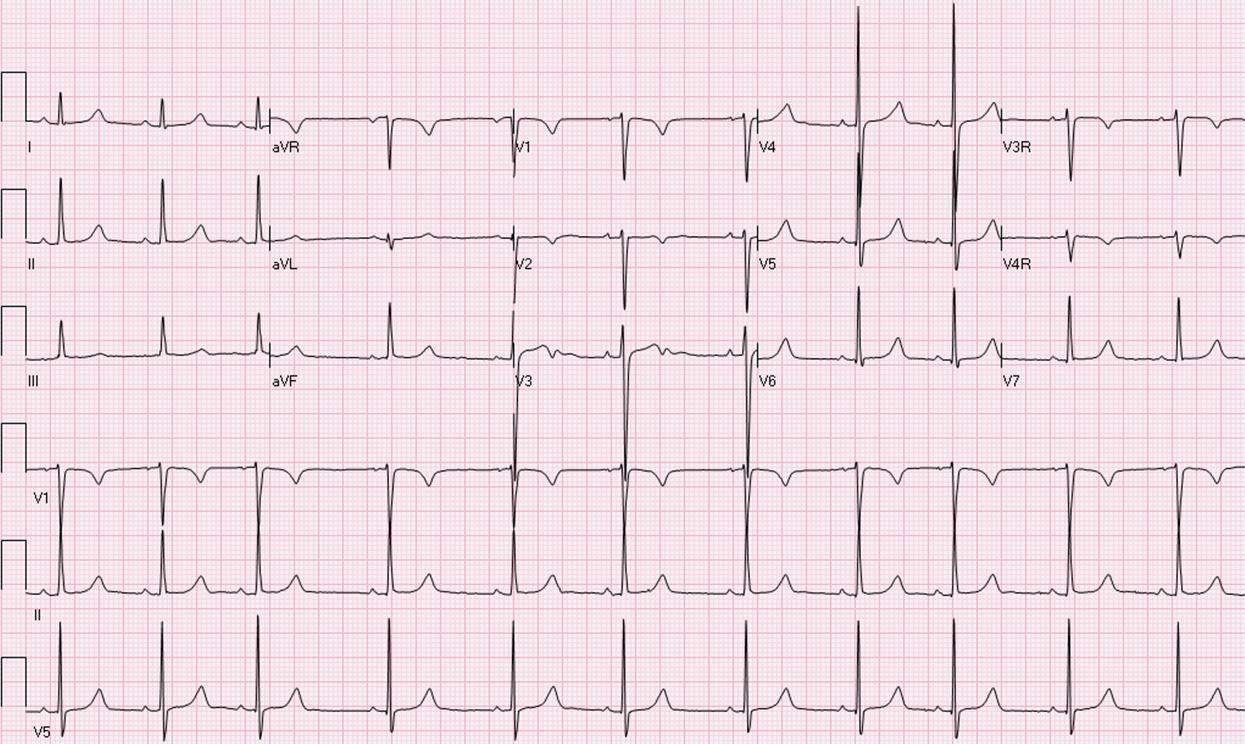
At her clinical evaluation her height is in the third percentile and weight is in the 10-25th percentile on an uncorrected growth curve. Her resting heart rate (HR) is 68 bpm and blood pressure is 107/72 mm Hg in her right arm and 119/57 mm Hg in her right leg. Her cardiac exam reveals a regular rate and rhythm, normal S1 and S2. A click is heard at the right upper sternal border (RUSB). She has a II/VI systolic ejection murmur at the RUSB and left upper sternal border (LUSB) with no radiation to her back. The remainder of her physical exam is normal. Her electrocardiogram (ECG) is shown (Figure 1). Her echocardiogram shows normal biventricular function, a functional bicuspid aortic valve with mild flow acceleration on color Doppler and a peak systolic gradient of 29 mm Hg (mean gradient of 16 mm Hg) across the aortic valve. There is no left ventricular (LV) hypertrophy, and the LV mass is normal. Her aortic root measurements by echocardiogram are shown below (Table 1). She underwent cardiovascular magnetic resonance imaging (MRI), which revealed normal ventricular volumes (LV mass indexed of 62.8 gm/m2, Z score 1.5). Her aortic measurements on magnetic resonance angiography (MRA) showed an aortic root of 2.6 x 3.0 cm and an ascending aorta of 3.0 x 3.2 cm. She also underwent a progressive exercise test on a treadmill using the Bruce protocol showing her to have a VO2 max of 43.5 mL/kg/min. at peak exercise (124% of predicted) and peak respiratory exchange ratio (RER) of 1.03. Her HR and blood pressure responded appropriately to exercise.
Table 1
|
|
Ao Root |
Ao Root Z score |
Asc Ao |
Asc Ao Z score |
Peak systolic gradient/Mean gradient |
BSA |
|
2009 |
2 cm |
0 |
2.47 cm |
2 |
32/14 |
1.11 |
|
2010 |
2.5 cm |
0.99 |
2.79 cm |
3.1 |
21/11 |
1.19 |
|
2012 |
2.53 cm |
0.4 |
3.07 cm |
3.84 |
24 |
1.36 |
|
2013 |
2.7 cm |
0.89 |
2.9 cm |
3.5 |
23/12 |
1.4 |
|
2014 |
2.75 cm |
1.2 |
3.4 cm |
5.1 |
29/16 |
1.39 |
Which of the following is the best management course for this patient?
Show Answer