A 19-year-old Caucasian female cross-country runner with no significant past medical history presents to a cardiology office for an evaluation as part of a routine screening program for varsity athletes at her university. This includes a 12-lead electrocardiogram (ECG) and a screening two-dimensional (2-D) echocardiogram.
On presentation, her only subjective complaint includes mild, non-exercise-limiting dyspnea with heavy exertion, and otherwise denies any chest pain, palpitations, dizziness, or syncope. She denies any drug or alcohol use. She has no family history of premature coronary disease, arrhythmias, heart failure, or sudden cardiac death. Her vitals and physical exam are unremarkable.
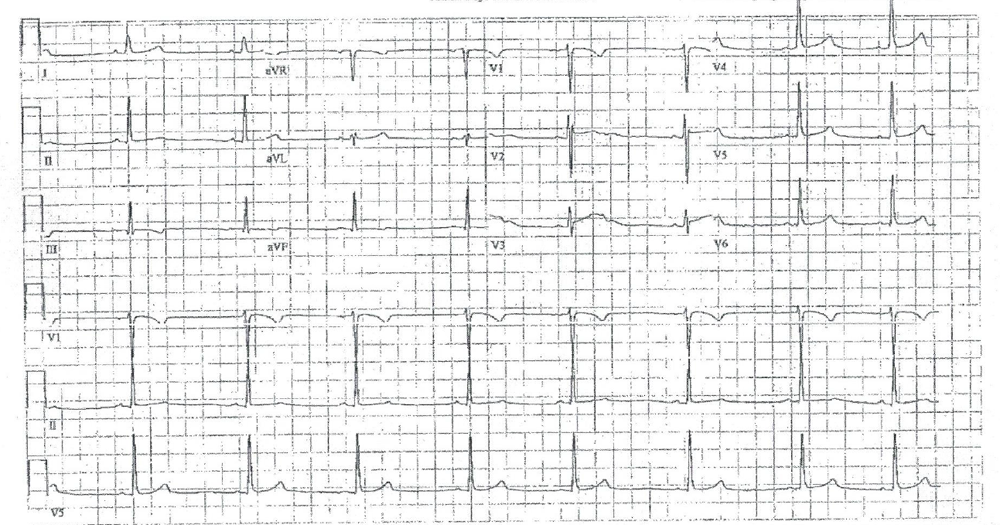
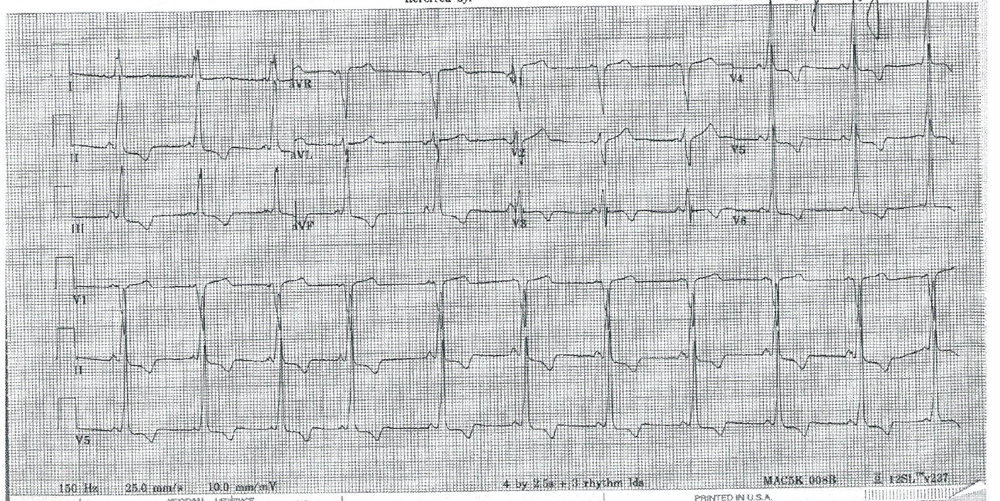
Figure 1 demonstrates an electrocardiogram (ECG) completed two months prior in her primary care physician's office. Figure 2 shows her in-office ECG that is completed as part of the screening program. Her screening 2-D echocardiogram is normal.
Which of the following describes the most appropriate next step?
Show Answer
The correct answer is: C. The patient should undergo noninvasive testing with Holter monitoring or exercise stress testing.
It is known that in patients with asymptomatic Wolff-Parkinson-White (WPW) syndrome, there is a small, but certain, risk of sudden unexplained death. In younger patients (<30 years of age), with asymptomatic WPW on ECG, there is an increased risk for the development of life-threatening arrhythmias. The Pediatric & Congenital Electrophysiology Society (PACES)/Heart Rhythm Society (HRS) expert consensus statement on the management of the asymptomatic young patient with a WPW ECG pattern provides a management algorithm to risk stratify these young patients, while the 36th Bethesda Conference Task Force guides management for competitive athletes.
Young patients who are not participating in competitive sports and demonstrate intermittent pre-excitation may be managed with cardiology observation and counseling regarding symptom awareness.1 There is an alternative approach to WPW management in competitive athletes. The 36th Bethesda Conference Task Force recommends a noninvasive assessment with a stress test and echocardiogram to assess for cardiovascular disease.2 Athletes without palpitations, tachycardia, or structural heart disease can participate in all competitive sports. An invasive electrophysiology study with radiofrequency ablation would be indicated in athletes with impaired consciousness, long-lasting palpitations, or rapid heart rates.
This case demonstrates a young, asymptomatic athlete who is incidentally found to have intermittent ventricular pre-excitation on a screening ECG and addresses the need for risk stratification in this patient. This patient underwent noninvasive testing with an exercise stress test, which demonstrated QRS prolongation with a slurred upstroke early in exercise (Stage 1) that completely resolved in Stage 3 of the Bruce Protocol. She remained asymptomatic and did not develop exercise-induced arrhythmias during her stress test. Loss of the WPW pattern at physiologic heart rates suggests that the effective refractory period of the accessory pathway is longer than that of the atrioventricular node: it would be unlikely for pre-excited atrial fibrillation to develop in this patient. Since she was, therefore, at lower risk for a lethal cardiac arrhythmia, further invasive studies and catheter ablation were deferred in her case unless she becomes symptomatic or develops structural heart disease.
References
Pediatric and Congenital Electrophysiology Society (PACES), Heart Rhythm Society (HRS), American College of Cardiology Foundation (ACCF), et al. PACES/HRS expert consensus statement on the management of the asymptomatic young patient with a Wolff-Parkinson-White (WPW, ventricular preexcitation) electrocardiographic pattern: developed in partnership between the Pediatric and Congenital Electrophysiology Society (PACES) and the Heart Rhythm Society (HRS). Endorsed by the governing bodies of PACES, HRS, the American College of Cardiology Foundation (ACCF), the American Heart Association (AHA), the American Academy of Pediatrics (AAP), and the Canadian Heart Rhythm Society (CHRS). Heart Rhythm 2012;9:1006-24.
Jere H. Mitchell, MD, William Haskell, PhD, Peter Snell, PhD and Steven P. Van Camp, MD. Task Force 8: classification of sports. J Am Coll Cardiol 2005;45:1364-1367.