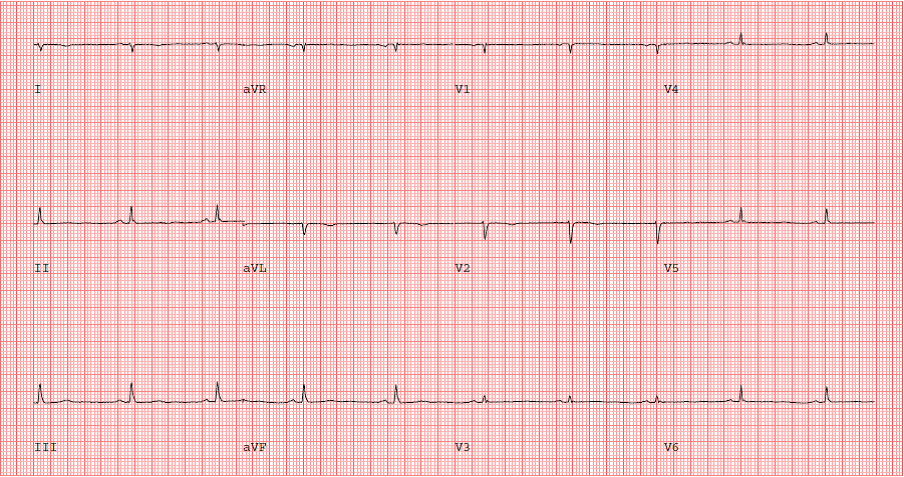
A 45-year-old woman presents to her primary care physician complaining of not feeling well with generalized fatigue and symptoms of major depression. She states that her mother died two months ago and her father had a stroke shortly afterwards. She also reports exertional dyspnea and chest tightness of several weeks duration. Her past medical history is significant for Grave's disease that was treated with total thyroidectomy, allergic rhinitis, major depression, and hyperlipidemia. Her medications include levothyroxine, escitalopram, and Flonase. On physical exam she was hemodynamically stable and afebrile, not in any acute distress, lungs clear to auscultation, heart sounds normal with regular rate and rhythm, no jugular venous distention noted, no lower extremity edema. She was referred for an exercise stress single-photon emission computed tomography myocardial perfusion imaging (MPI) study to further evaluate her symptoms. Her resting ECG is shown (Figure 1).
Figure 1: Resting ECG
She completed stage 3 on the Bruce protocol achieving a peak heart rate and blood pressure of 144 beats/min and 186/57 mm Hg, respectively. She reported no chest pain and test was stopped due to fatigue. The stress ECG and MPI images are shown (Figures 2 and 3).
Figure 2: ECG at peak exercise
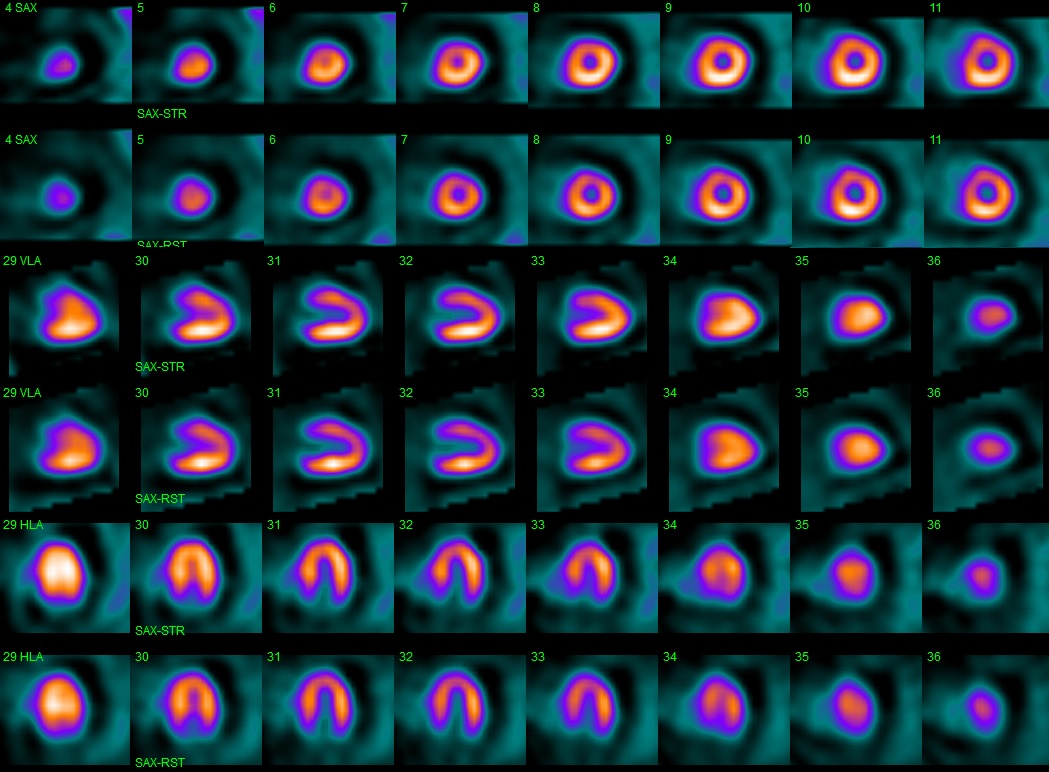
Figure 3: MPI images (stress)
What is the best next step in management of the patient?
Show Answer
The correct answer is: D. Echocardiography.
The patient's MPI did not reveal any perfusion defects to suggest coronary artery disease, therefore options A and B are incorrect. The images are of adequate quality. There is no reason to perform PET imaging. On the MPI images there is a halo of hyperlucency around the heart suggestive of a large pericardial effusion. The swinging motion of the heart can be seen in the gated images (Video A).
Video A
The patient was hemodynamically stable without any clinical signs of tamponade. An emergent echocardiogram was performed confirming the presence of a large pericardial effusion but there were no signs of tamponade (Video B).
Video B
Serum TSH was severely elevated at 120µIU/ml. The patient admitted to non-adherence to levothyroxine therapy since her mother's death and the intensification of her depressive symptoms. Over the next several months her TSH trended down towards normal with levothyroxine treatment. The patient was managed conservatively with close follow-up and serial echocardiograms but her symptoms persisted and she underwent elective pericardiocentesis draining more than 700 ml of fluid. The pericardial effusion was greatly diminished after the pericardiocentesis (Video C). Her shortness of breath improved but her fatigue and depression persisted.
Video C
It is important to assess for and appreciate the presence of extra-myocardial findings when interpreting MPIs. In many instances significant findings can be detected that impact the clinical management of the patient and occasionally these findings are related to the symptoms that initiated the work-up. In addition to pericardial effusion, an enlarged dysfunctional right ventricle suggestive of pulmonary embolism, and lungs, breast, thyroid and thymus cancers have been detected on MPI.