A 48-year-old black female was transferred for further evaluation of chest pain and abdominal free air. The patient initially presented with substernal chest pain, described as exercise induced chest pressure with associated right arm radiation and dyspnea, relieved with rest. During the five days prior to evaluation the symptoms increased in frequency, progressing to rest pain. The initial emergency department ECG was without ischemic changes.
Past medical history included untreated hypertension, tobacco use and family history of premature disease, appendectomy, and hysterectomy, both greater than five years prior to admission.
Initial TnI was normal. A chest CT was performed to exclude pulmonary embolism. No embolism was seen; however, there was demonstrated significant sub-diaphragmatic free air. Repeat physical exam demonstrated no abdominal tenderness, rebound, guarding, or other symptoms referable to the abdomen.
The patient was transferred for further evaluation. Physical exam at arrival showed a blood pressure 110/70 mmHg, heart rate 70 bpm, normal lung exam, cardiac exam was regular rate and rhythm without murmurs or gallop. The abdominal exam demonstrated normal bowel sounds, non-tender, non-distended without guarding or rebound, and no edema.
Laboratory values:
Figure 1
BUN/Cr: normal
Serial TnI (-) over 18 hours, with all values <0.03 ng/ml (lowest value reported by the lab).
Serial ECGs demonstrated significant anterior T-wave inversion (Figure 1).
An echocardiogram demonstrated mild and distal anterior septal hypokinesis.
Abdominal CT confirmed the free air, without evidence of bowel obstruction. Given the location, gastric or duodenal perforation was considered the most likely etiology, as there had been no recent abdominal instrumentation.
Surgical consult was obtained; the recommendation was against any anti-platelet agent including aspirin, heparin and clopidogrel.
Treatment was started with beta-blockers, nitrates intravenously, and low dose calcium channel blocker.
What do you think is the most likely etiology for the ECG changes?
Show Answer
The correct answer is: C. Wellen's Syndrome
The patient’s symptoms, the evolution of the ECG changes and the wall motion abnormalities on the echocardiogram were thought to be most consistent with a diagnosis of unstable angina with associated proximal left anterior descending stenosis1.
Wellen’s Syndrome1 was first reported in 1982. Of 145 patients consecutively admitted for unstable angina, 26 (18%) showed deep anterior T wave inversion. In spite of symptom control 12 of 16 patients (75%) who were not operated on developed extensive anterior wall infarction within a few weeks after admission.
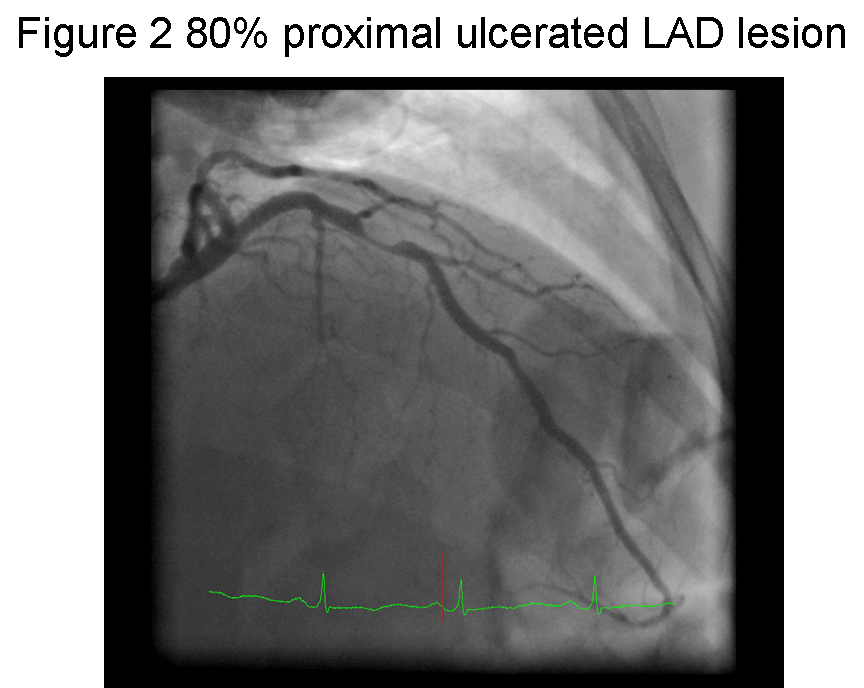
Figure 2
This case illustrates that even with current sensitive Tn, patients can present with myocardial ischemia without detectable necrosis. It is likely in the future the number of patients with ischemia without infarction will be reduced as use of very high sensitivity Tn assays increases2, which may have elevated in this patient.
case2_111610Because of the abdominal free air, and potential need for surgery, urgent risk stratification was indicated, and we chose to perform coronary angiography, which demonstrated a significant proximal 80% ulcerated left anterior descending stenosis (figure 2).
Although abdominal perforation could be consistent with significant mental stress, resulting in a Takotsubo cardiomyopathy, typically it is associated with Tn elevations and significant anterior septal and apical wall motion abnormalities3. In our patient, the wall motion abnormalities were not severe, and there was no detectable TnI. Takotsubo cardiomyopathy is usually considered a diagnosis of exclusion and requires the presence of relatively normal coronary arteries which can't be demonstrated without coronary angiography or CT angiography, and further imaging of the coronaries is necessary. Given these findings, Takotsubo cardiomyopathy was considered unlikely, and unstable angina was considered the most likely cause.
Significant ECG changes have been associated with a number of abdominal conditions, including pancreatitis4 and cholecystitis. Whether this results from a Takotsubo-like syndrome and is purely and ECG-related phenomenon4 has not been well investigated. The absence of any abdominal symptoms and associated wall motion abnormalities were thought to make this unlikely.
The rationale for performing coronary angiography was that there was no significant stenosis and further evaluation, including surgery if necessary, could proceed with minimal risk to the patient. The presence of significant coronary disease would necessitate greater precautions prior to further abdominal evaluation. Revascularization without further defining the abdominal process was thought be contraindicated given the risks of required dual platelet therapy. CT angiography would be a reasonable alternative to coronary angiography.
Coronary angiography was chosen, as stress echocardiography either with exercise or dobutamine was thought to be unsafe due to the ECG changes related to severe coronary disease. Pharmacologic stress MPI would be lower risk, but given the high pre-test probability, further testing with coronary diagnostic angiography, without intervention, was thought the best way to proceed.
The patient subsequently underwent an upper GI that was negative; upper endoscopy also failed to reveal the site of perforation. It was thought the perforation had spontaneously sealed. She subsequently underwent uncomplicated LAD stenting four days after admission, and was discharged the next day on dual anti-platelet treatment, without further complication.
References
de Zwann C, Bar FW, Wellens HJJ: Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J 1982;103:730-736.
Wilson SR, Sabatine MS, Braunwald E, Sloan S, Murphy SA, Morrow DA. Detection of myocardial injury in patients with unstable angina using a novel nanoparticle cardiac troponin I assay: observations from the PROTECT-TIMI 30 Trial. Am Heart J. 2009;158:386-91.
Sharkey SW, Windenburg DC, Lesser JR, et al. Natural history and expansive clinical profile of stress (tako-tsubo) cardiomyopathy. J Am Coll Cardiol. 2010;55:333-41.
Khairy P, Marsolais P Pancreatitis with electrocardiographic changes mimicking acute myocardial infarction. Can J Gastroenterol. 2001;15:522-6.