A 53-year-old man with multiple cardiac risk factors but no previously documented coronary artery disease reports intermittent, non-exertional chest discomfort during a routine visit to his primary physician. A stress test with imaging is performed. This study does not reveal any electrocardiogram (ECG) or perfusion abnormalities with diagnostic workload. The patient's symptoms persist, and he undergoes cardiac catheterization at an outside hospital. The report of this study indicates that no epicardial stenoses are visible, but that aneurysms are present in the left anterior descending (LAD) artery and the right coronary artery (RCA). Shortly after this study is performed, the patient is started on a beta-blocker, aspirin, and warfarin and is referred for further management.
The patient's symptoms improve after initiation of medical therapy but do not disappear. His physicians, therefore, perform cardiac computed tomography angiography (CTA), which confirms that the proximal LAD contains a large, eccentric aneurysm extending to the first diagonal branch (Figure 1). The maximum luminal diameter of the aneurysmal segment was 15 mm. A mural thrombus was present, and the maximum external diameter of this segment was 27 mm. Focal aneurysms <10 mm in diameter were also observed in the left circumflex artery. The RCA was diffusely ectatic along its entire length, with a maximum diameter of 12 mm. There was no evidence of atherosclerotic disease.
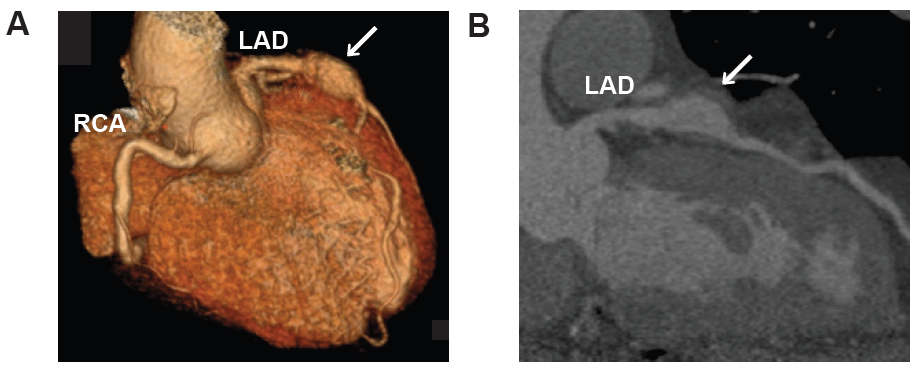
Figure 1: Coronary Artery Aneurysms
Panel A contains a three-dimensional reconstruction of the CTA, in which the RCA and LAD artery are visible. The aneurysmal segment of the LAD is focal and is indicated with an arrow. The RCA contains a long, tubular aneurysm.
Panel B contains a curved reformat view of the LAD in which the aneurysmal segment is indicated with an arrow. The tip of this arrow is in contact with the outer wall of the aneurysm, which is separated from the inner lumen by mural thrombus.
CTA = computed tomography angiography; LAD = left anterior descending; RCA = right coronary artery.
A CTA of the head and neck is performed and reveals no arterial aneurysms or other vascular anomalies. A magnetic resonance angiogram of the chest confirms that the caliber of the thoracic aorta is normal with no aneurysmal segments. The proximal segments of the aortic branches are similarly normal in appearance. There are also no abnormalities in the visceral arteries or in the arteries of the extremities. In addition, none of these studies demonstrate any evidence of atherosclerotic disease. Extensive laboratory testing is performed, and molecular markers of connective tissue disease and active inflammation are negative.
Which of the following describes the most likely etiology of the coronary aneurysms in this patient?
Show Answer
The correct answer is: D. Kawasaki disease.
Coronary artery aneurysms (CAAs) are defined as being focal segments of coronary arteries that are dilated to at least 1.5 times the normal diameter. Estimates of the incidence of CAAs are based on a small number of observational studies and are quite variable. In most studies, the reported incidence of CAAs ranges from 0.3 to 5.3%.1-4 One study from India reported an incidence of 10-12%.5 It has been suggested that these differences may reflect differences in hereditary and environmental risk factors among the patient groups studied.6,7 The most commonly affected vessel is the RCA, followed by the LAD. Involvement of the left main coronary artery is rare.8
Approximately 50% of CAAs in adults are attributable to atherosclerosis.9 It follows that patients with coronary aneurysms are more likely to be male and to have hyperlipidemia.10 The patient described in this case was at risk for CAD, but there was no evidence of atherosclerosis on the coronary angiogram and subsequent CT imaging. Therefore, it is unlikely that his aneurysms could be the result of atherosclerosis.
Congenital anomalies are responsible for up to 30% of CAAs.8 Extensive cardiac imaging in this patient did not reveal any congenital anomalies of the heart. In addition, there was no evidence of congenital anomalies of the cardiac or peripheral arteries. Therefore, it is not possible to invoke a congenital anomaly as the cause of this patient's coronary aneurysm.
Approximately 15% of CAAs are caused by inflammatory disorders, including vasculitides and connective tissue disorders.8 Takayasu arteritis is a systemic vasculitis that affects primarily females.11 Patients with Takayasu arteritis often present with an acute inflammatory phase, followed by a chronic phase. During the chronic phase, patients typically bear clinical manifestations of the stenosis and/or occlusion of large cardiac vessels, notably the aorta and its branches. Coronary artery aneurysms secondary to Takayasu arteritis have been reported but are rare. The patient described in this report did not present with any evidence of an acute inflammatory process, nor did his extensive vascular imaging reveal any evidence of stenosis or occlusion of large arteries. Therefore, his presentation is not consistent with the typical manifestations of Takayasu arteritis.
Kawasaki disease is a systemic vasculitis syndrome that affects predominantly children and is known to precipitate CAA formation. Up to 10-15% of children with Kawasaki disease present with vasculitis of the small and medium size arteries, with frequent involvement of the coronary arteries.12 The incidence of Kawasaki disease is highest in Japan, and family history has been identified as a risk factor.13 A single causative factor has not been identified, but gamma globulin treatment has been shown to be effective. Up to 25% of untreated children develop persistent CAAs.14 Because many cases of Kawasaki disease are unidentified in the acute phase, these CAAs can be found incidentally in adulthood. The patient described in this case did not have identified Kawasaki disease in childhood. He did, however, report frequent viral syndromes during his childhood, one of which involved high fever, severe pharyngitis, and glossitis. He did not receive care from a physician for this illness, which was suspected to be unidentified Kawasaki disease. The CAAs in this patient were, therefore, considered to be secondary to prior Kawasaki disease.
References
Hartnell G, Parnell B, Pridie R. Coronary artery ectasia. Its prevalence and clinical significance in 4993 patients. Br Heart J 1985;54:392-5.
Swaye P, Fisher L, Litwin P et al. Aneurysmal coronary artery disease. Circulation 1983;67:134-138.
Demopoulos V, Olympios C, Fakiolas C, et al. The natural history of aneurysmal coronary artery disease. Heart 1997;78:136-41.
Baman T, Cole J, Devireddy C, Sperling L. Risk factors and outcomes in patients with coronary artery aneurysms. Am J Cardiol 2004;93:1549-51.
Sharma S, Kaul U, Sharma S, et al. Coronary arteriographic profile in young and old Indian patients with ischaemic heart disease: a comparative study. Indian Heart J 1990;42:365-9.
Cohen P, O'Gara PT. Coronary artery aneurysms: a review of the natural history, pathophysiology, and management. Cardiol Rev 2008;16:301-4.
Dahhan A. Coronary artery ectasia in atherosclerotic coronary artery disease, inflammatory disorders, and sickle cell disease. Cardiovasc Ther 2015;33:79-88.
Swanton R, Thomas M, Coltart D, Jenkins B, Webb-Peploe M, Williams B. Coronary artery ectasia--a variant of occlusive coronary arteriosclerosis. Br Heart J 1978;40:393-400.
Daoud A, Pankin D, Tulgan H, Florentin R. Aneurysms of the coronary artery. Report of ten cases and review of literature. Am J Cardiol 1963;11:228-37.
Sudhir K, Ports T, Amidon T, et al. Increased prevalence of coronary ectasia in heterozygous familial hypercholesterolemia. Circulation 1995;91:1375-80.
Lim A, Lee G, Jang S, et al. Gender differences in clinical and angiographic findings of patients with Takayasu arteritis. Clin Exp Rheumatol 2015;33(2 Suppl 89):S132-7.
Newburger J, Takahashi M, Burns J, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med 1986;315:341-7.
Nakamura Y, Yashiro M, Uehara R, Oki I, Watanabe M, Yanagawa H. Epidemiologic features of Kawasaki disease in Japan: results from the nationwide survey in 2005-2006. J Epidemiol 2008;18:167-72.
Rowley A, Baker S, Orenstein J, Shulman S. Searching for the cause of Kawasaki disease--cytoplasmic inclusion bodies provide new insight. Nat Rev Microbiol 2008;6:394-401.