A 64-year-old diabetic, hypertensive woman was found to be in persistent atrial fibrillation on routine examination. Despite an initial rate control strategy with combination carvedilol and diltiazem, she continued to have high ventricular rates ranging from 90 to 130 beats a minute.
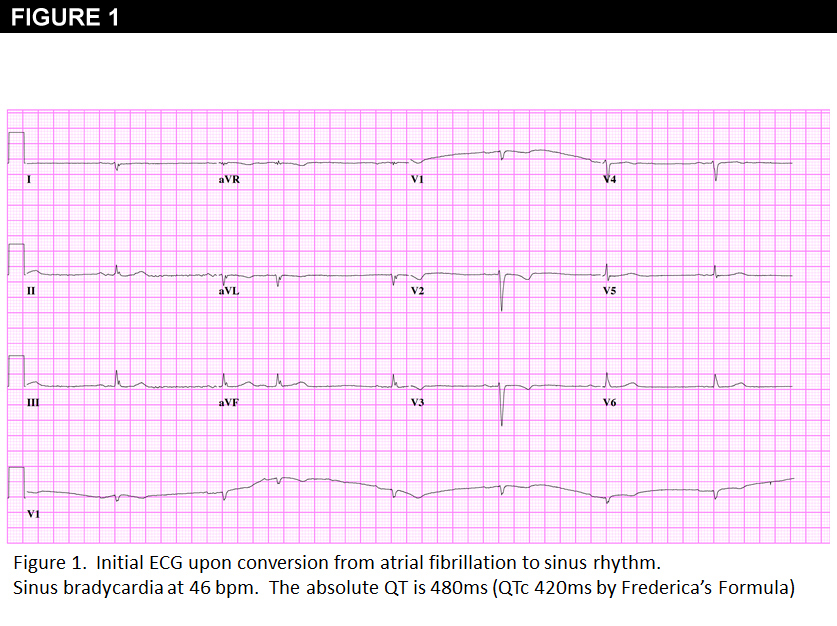
A transthoracic echocardiogram revealed mild concentric left ventricular hypertrophy with an LV wall thickness of 1.1cm and an ejection fraction of 55%. Her estimated creatinine clearance was 72.5 mL/min (based on a creatinine of 1.2mg/dL and a weight of 97.2kg [213 lbs; BMI = 42]), potassium 3.7 mmol/L and magnesium 1.7 mmol/L. She was admitted for initiation of Sotalol and cardioversion. Carvedilol and diltiazem were discontinued. After 4 doses of sotalol at 80mg twice daily (under telemetric monitoring), she converted to sinus bradycardia at 46 bpm and a QTc of 420 ms (Figure 1). She was discharged home (on sotalol 80mg twice daily), with follow up scheduled in a week’s time. Six days later, the patient developed recurrent presyncope, ultimately culminating in an abrupt episode of syncope just after showering at a rehabilitation center.
What would you recommend next?
Show Answer
The correct answer is: C. Refer to emergency department for repeat ECG
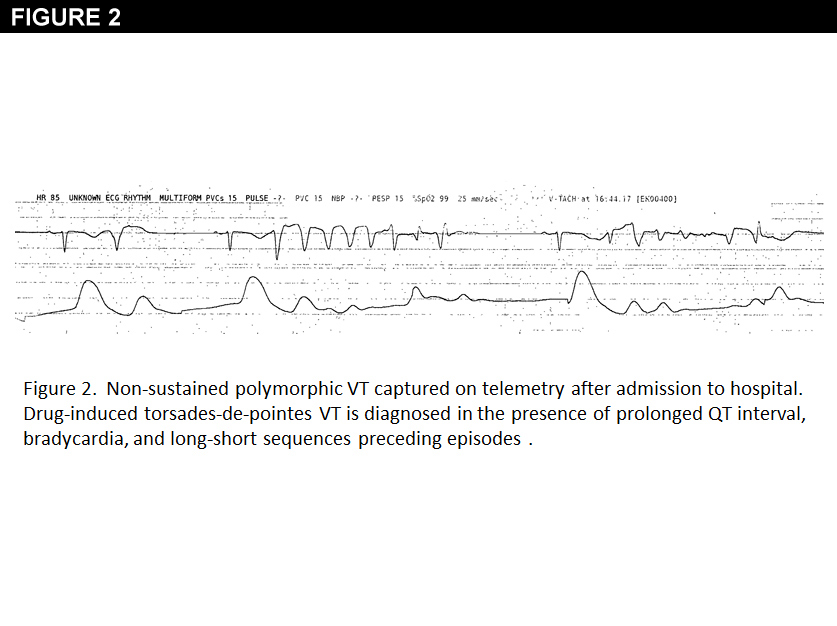
Upon presentation to hospital, she was found to have recurrent non-sustained salvos of polymorphic ventricular tachycardia (VT) (Figure 2), with a prolonged QT interval (Figure 3).
This is a case of drug-induced torsades de Pointes (TDP) ventricular arrhythmia due to sotalol. As is often the case, the polymorphic VT episodes were symptomatic and non-sustained, but place the patient at significant risk of sudden death. A full history and biochemical profile did not reveal any obvious predisposing factors. Her estimated creatinine clearance was unchanged and her potassium and magnesium levels remained within normal range. She had no prior history of syncope, was on no QT prolonging agents and had no family history of sudden death.
The reported incidence of TDP from sotalol varies from 1% to 4%(1). QT prolongation is linearly related to plasma concentration, and since sotalol is mainly cleared by the kidneys, renal dysfunction is a particularly significant risk factor. Elimination half-life increases from 8 hours in patients with normal renal function to 24 hours in those with moderate renal insufficiency(2). When used for the treatment of atrial fibrillation, sotalol is contraindicated when the creatinine clearance is less than 40 mL/min. Standard equations for calculating creatinine clearance, such as Cockcroft-Gault, may overestimate creatinine clearance in morbidly obese patients such as ours, which may partially account for the late presentation after an unremarkable standard monitoring period(3).
Female gender has also been identified as an independent predictor of risk(4,5). In comparison to males, females generally have a longer baseline QT interval, and have a greater response to IKr blocking agents, potentiating the risk of an arrhythmic complication. Other factors such as a history of heart failure or coronary heart disease, hypokalemia, hypomagnesemia, and the concomitant use of other QT prolonging drugs may also contribute to the risk of torsades.
Sotalol is a class III antiarrhythmic agent that blocks beta- adrenergic receptors and the IKr potassium channel. IKr mediates the rapid component of the delayed rectifier potassium current. Sotalol prolongs repolarization by inhibiting IKr, thereby prolonging the QT interval. This extended period of repolarization allows for early after-depolarizations that trigger torsades de pointes. In the case of IKr blockers, QT prolongation tends to be more pronounced at slower heart rates, as was the case in our patient(5).
Therefore, although current guidelines suggest that outpatient initiation of sotalol remains a reasonable approach in those without obvious risk factors and a baseline QT less than 450ms(6), this case reflects the importance of continued vigilance due to delayed risk of proarrhythmia, particularly in women and those with renal dysfunction or bradycardia. Despite the many benign causes of presyncope or syncope in the elderly, those presenting with these symptoms following the initiation of antiarrhythmics should be evaluated immediately.
This patient was admitted to hospital for monitoring. Sotalol was immediately discontinued. A permanent pacemaker was implanted to correct persistent sinus bradycardia and facilitate an aggressive rate control strategy. Initiating a class I antiarrhythmic, such as flecainide or propafenone, would also have been a reasonable approach, but LVH was present. Antiarrhythmics, such as dofetilide and dronedarone also prolong the QT interval and would be contraindicated. Although amiodarone may also lengthen the QT, it very rarely results in TDP. Pulmonary vein isolation or AV node ablation with concurrent pacemaker (or CRT) implant could also be considered.
References
Soyka LF, Wirtz C, Spangenberg RB. Clinical safety profile of sotalol in patients with arrhythmias. Am J Cardiol 1990; 65:74A
Blair AD, Burgess ED, Maxwell BM, Cutler RE. Sotalol kinetics in renal insufficiency. Clinical Pharmacology and Therapeutics 1981; 29:457–463; doi:10.1038/clpt.1981.63
Demirovic JA, Pai AM, Pai MP. Estimation of Creatinine Clearance in Morbidly Obese Patients. AJHP 2009; 66:642-648
Lehmann MH, Hardy S, Archibald D, quart B, MacNeil DJ. Sex difference in risk of torsade de pointes with d,l-sotalol. Circulation 1996; 94:2535
Roden DM. Drug-Induced Prolongation of the QT Interval. N Engl J Med 2004; 350:1013-22
Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al. 2011 ACCF/AHA/HRS focused updates incorporated Into the ACC/AHA/ESC 2006 Guidelines for the management of patients With atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in partnership with the European Society of Cardiology and in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. J Am Coll Cardiol 2011; 57:e101-198.