54-year-old male with a past history significant for hyperlipidemia, hypertension, and chronic reflux esophagitis presented with episodes of mid sternal chest pain associated with mild shortness of breath, aggravated by cough. The patient was active and well until about a month prior when he had flu-like illness with similar chest pain, which progressed to worsening fatigue, pedal edema, and NYHA class II-III symptoms.
Clinical examination revealed an elevated jugular venous pulse to the angle of jaw and 2+ bilateral pedal edema. Auscultation revealed normal dual heart sounds with no rub or murmurs and mild bilateral basal crackles.
Further laboratory investigation was negative for infectious serology and only significant for raised CRP of 244 mg/L.
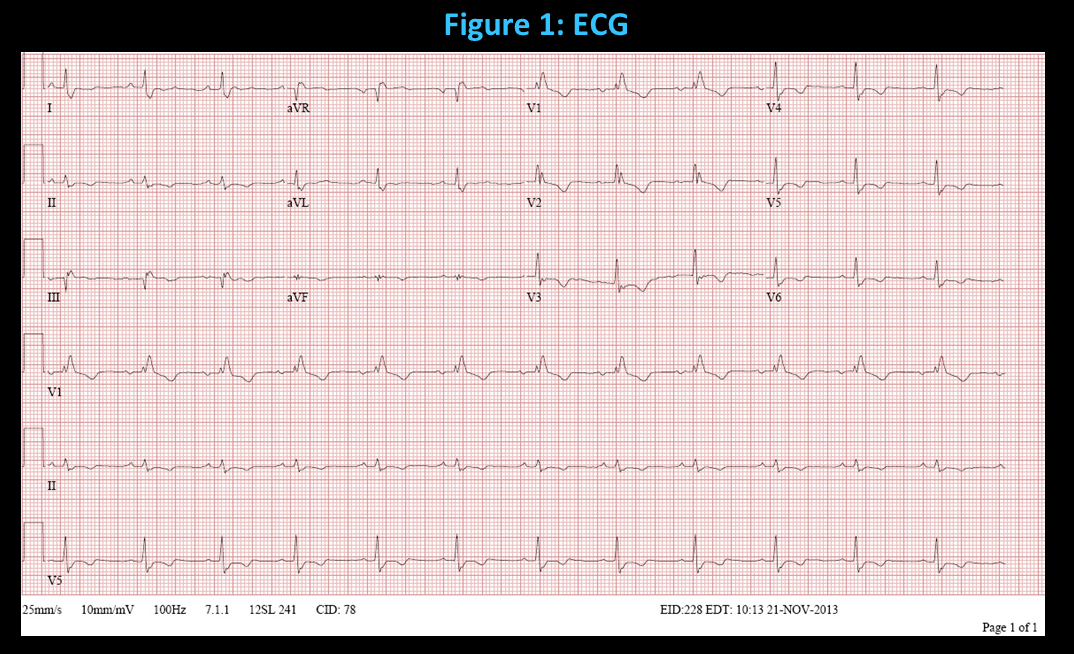
The ECG, echocardiography and cardiac MRI images are shown (Figure 1 – Figure 4), which were acquired at the time of initial consultation.
What is the most likely clinical diagnosis and next best step in management?
Show Answer
The correct answer is: D. Constrictive pericarditis requiring a trial of medical therapy.
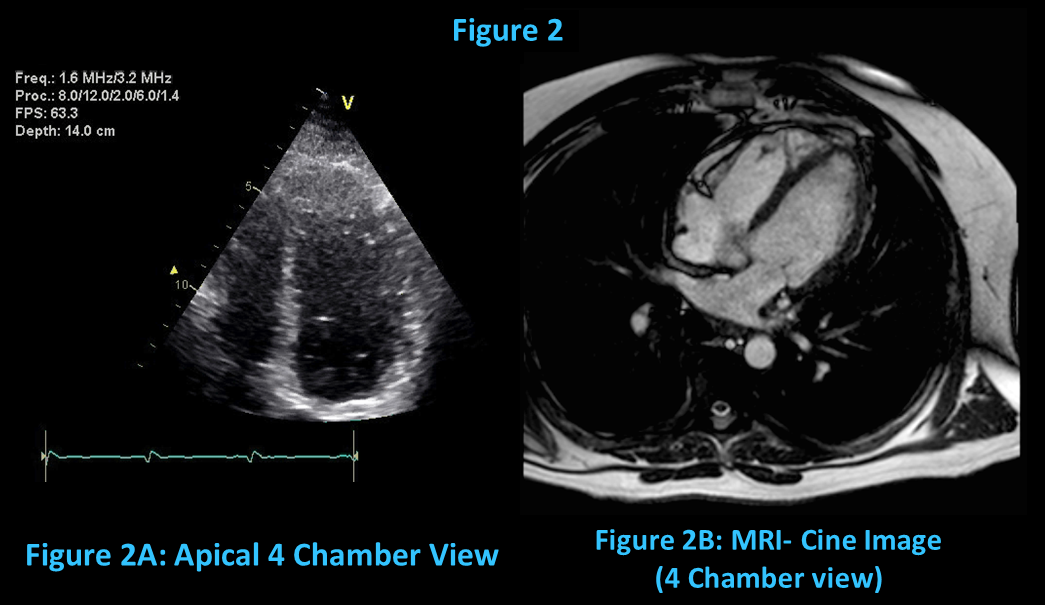
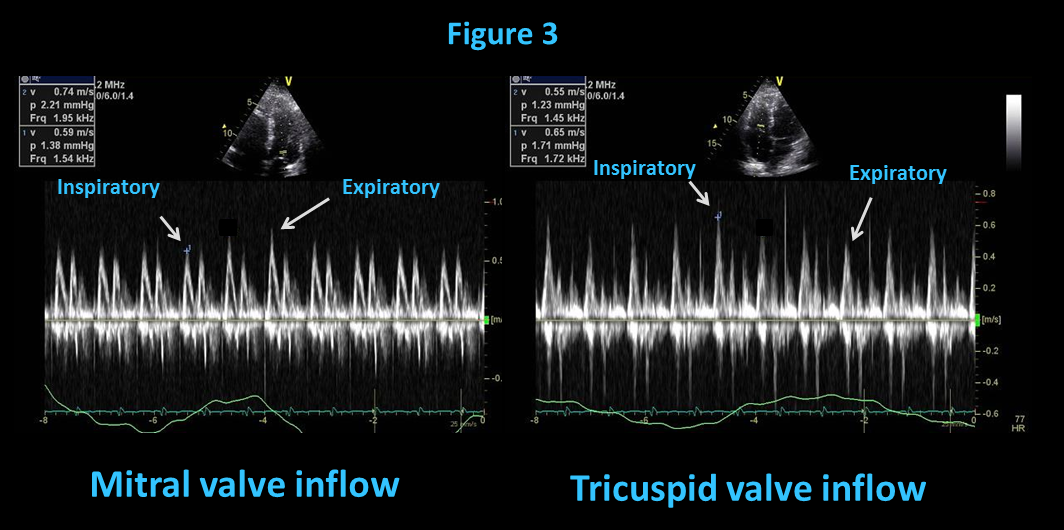
The patient was diagnosed with Transient constrictive pericarditis (CP). ECG reveals RBBB with diffuse global T wave inversion (Figure 1), and initial echocardiography (Figure 2A) depicts significant diastolic septal bounce, tethering of the right ventricular apex with early features of left ventricular conical deformity. Also, there is a restrictive mitral valve inflow pattern with significant respirophasic variation of mitral (reduced inspiratory inflow velocity of >25%) and tricuspid (increased inspiratory inflow velocity of >45%) valve inflow velocities (Figure 3), as well as exaggerated end-expiratory diastolic hepatic venous flow reversal (ratio of diastolic backward/systolic forward flow of >0.8 cm). Overall, this constellation of features is suggestive of inter-ventricular interdependence with constrictive physiology.
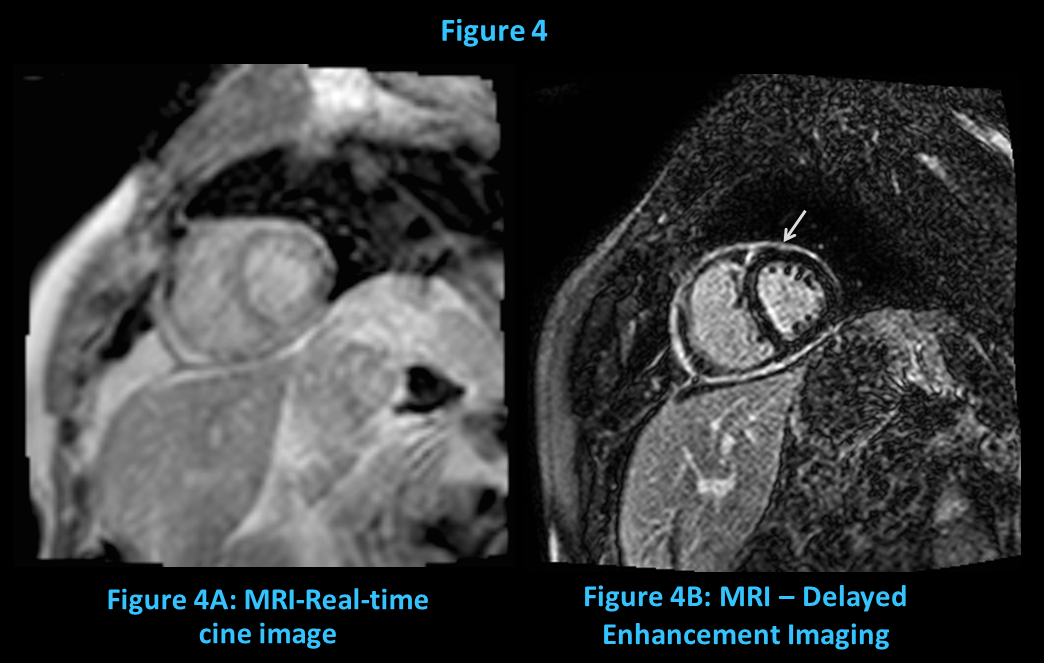
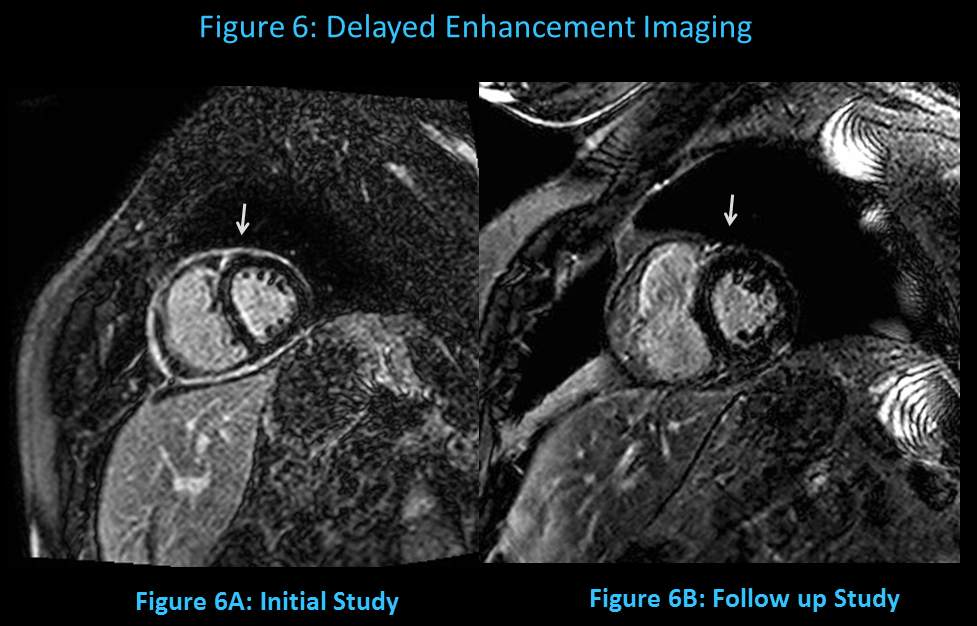
Furthermore, cardiac MRI (Figure 2B) reveals features already depicted by echocardiography, additionally the delayed enhancement imaging shows circumferentially increased pericardial delayed enhancement supporting the diagnosis of acute/sub-acute pericardial inflammation (Figure 4B). Again seen are mild right ventricular tethering near the apex, significant diastolic septal bounce and real time gradient echo cine imaging exhibiting inspiratory septal flattening (Figure 4A), all-consistent with underlying constrictive physiology.
Our patient was successfully treated according to the institutional guideline for treatment of pericarditis with a tapering dose of prednisone, NSAID and colchicine, along with pantoprazole with excellent clinical improvement.
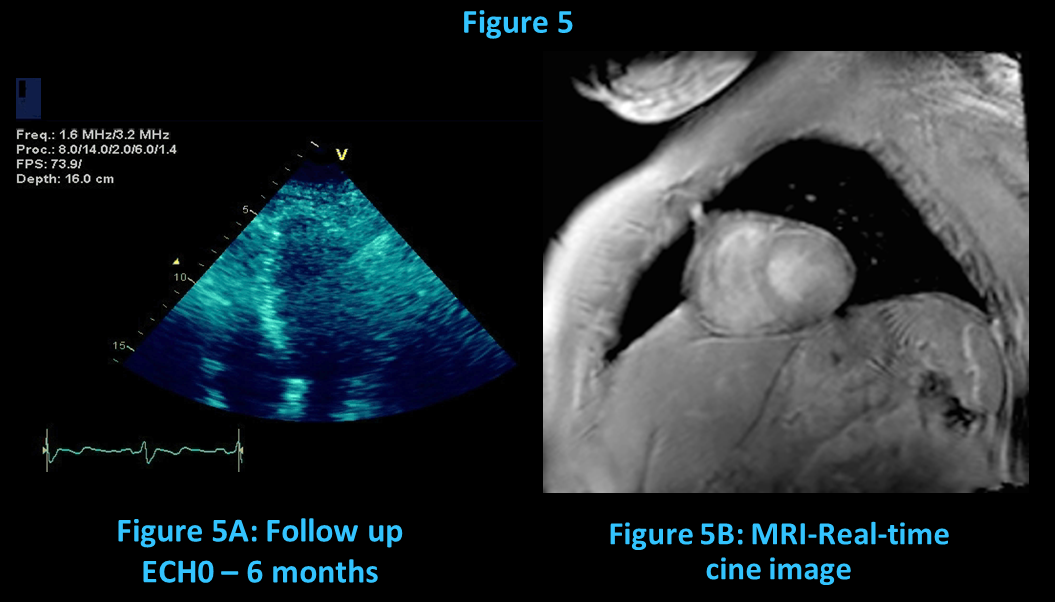
Follow-up echocardiography (Figure 5A) in 6 months revealed normalization of diastolic septal bounce, trans-mitral and tricuspid velocities, and resolution of right ventricular tethering. A repeat cardiac MRI also revealed resolution of delayed enhancement (Figure 5B) and respirophasic shift of the inter-ventricular septum (Figure 6).
The echocardiograph did not reveal any evidence of pericardial effusion (response A) and though our patient may have acute pericarditis (response B) there were additional features suggestive of constrictive physiology. Finally response C is partially correct with the right diagnosis, though surgical pericardiectomy is not an initial treatment option for transient CP before aggressive medical therapy.
TRANSIENT PERICARDITIS.
Transient constrictive pericarditis (CP) is described as development of hemodynamic features consistent with constriction physiology and subsequently resolves with medical therapy.
Transient CP was first described by Sagrista et al1 in 1987 in a group of 16 patients. Since then this phenomenon has been described in the literature with multiple case series and reviews, and has now been officially recognized as a variant of constrictive pericarditis by the European Society of Cardiology2. There are two forms of pericardial constriction when seen from a pathology standpoint, one being elastic and the other being a hard shell as was initially proposed by Hancock et al in 19803. It is the fibro-elastic form that represents the acute or sub-acute phase of constriction, where patients present with more subtle clinical features of constriction compared to the classic constrictive pericarditis. It was thought that the mechanism responsible for this finding was transiently thickened and inelastic pericardium resulting from edema and inflammation that subsequently resolved with anti-inflammatory treatment and observation. However, this may also represent an early manifestation in the spectrum of classic constrictive pericarditis that if untreated, results in chronic inflammation leading to fibrin and collagen deposition and thus permanent constrictive physiology.
Patients with transient CP are managed with anti-inflammatory therapy with a combination of a NSAID and colchicine. Steroid therapy should only be added in refractory cases, as the risk of recurrent pericarditis increases with the use of steroids especially if viral in etiology4. The time to normalization of the constrictive hemodynamics varies with an average of 8.3 weeks5, however this is from a subset 22 patients and larger multicenter studies are needed to know the natural history of this variant. In rare situations, patients may need steroid sparing therapy, such as anakinra or azathioprine, to over come the detrimental effects of long term steroids.
In conclusion, early recognition of transient CP can allow quicker initiation of effective anti-inflammatory therapy and to prevent the long-term transition into permanent/classic constrictive pericarditis.
References
Sagrista-Sauleda J, Permanyer-Miralda G, Candell-Riera J, Angel J, Soler-Soler J. Transient cardiac constriction: an unrecognized pattern of evolution in effusive acute idiopathic pericarditis. Am J Cardiol 1987;59:961-6.
Adler Y, Charron P, Imazio M et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015.
E.W. Hancock. On the elastic and rigid forms of constrictive pericarditis. Am Heart J, 100 (1980), pp. 917–923.
Imazio M, Bobbio M, Cecchi E, Demarie D, Demichelis B, Pomari F, Moratti M, Gaschino G, Giammaria M, Ghisio A, Belli R, Trinchero R. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial. Circulation. 2005;112:2012–2016
Haley JH, Tajik AJ, Danielson GK, Schaff HV, Mulvagh SL, Oh JK. Transient constrictive pericarditis: causes and natural history. J Am Coll Cardiol 2004;43:271-5