Thank you for visiting ACC.org. Please note that this item was published more than 5 years ago and therefore its content may be outdated. For more current information on this topic, we encourage you to visit our Congenital Heart Disease and Pediatric Cardiology Collection page.
A 12-month old, 11 kg, previously healthy, asymptomatic female was seen in the cardiology clinic for a persistent heart murmur. On physical exam, she had a Grade III/VI unusually low-pitched continuous murmur heard best along the lower left sternal board without radiation.
An echocardiogram demonstrated a large circular echo bright intracardiac mass measuring 14mm x 15mm that appeared to attach to the endocardium by a broad base along the right ventricular side of the interventricular septum, just below the tricuspid septal leaflet (Videos 1 and 2), with the potential for tricuspid inflow obstruction. The bi-ventricular size and systolic function were normal. There was trivial tricuspid regurgitation, with no right ventricular outflow obstruction. No other structural cardiac abnormalities were seen.
Cardiac MRI (cMRI) was performed which also demonstrated a large right ventricular mass on the septal side of the basal right ventricular chamber, in close proximity to the tricuspid valve apparatus (Video 3). Holter monitoring showed normal sinus rhythm throughout.
Video 1
Two-dimensional and color Doppler of the tricuspid valve in an apical four-chamber view. A large, circular echobright structure appears adherent to the septal leaflet of the tricuspid valve. There is mild tricuspid regurgitation, but now inflow obstruction.
Video 2
Two-dimensinoal view of the tricuspid valve in a parasternal long axis view. A large, circular echobright structure measuring 18 x 18 mm is seen. It appears adherent to the septal leaflet of the tricuspid valve and moves in concert with the valve apparatus.
Video 3
Cardiac MRI. After administration of contrast, a T1-weighted black blood image in the short axis reveals a peripherally enhancing mass at the basal portion of the right ventricle, measuring approximately 18 x 18 mm.
Which of the following is the most appropriate next step in the management of this patient?
Show Answer
The correct answer is: C. Complete operative resection of the mass on cardiopulmonary bypass.
Cardiac tumors in children are rare, with an autopsy frequency of 0.001% to 0.30%. Most primary cardiac tumors are benign, with rhadomyoma, myxoma, teratoma, and fibroma being most common. Papillary fibroelastoma is the third most common tumor in adults but is very rare in children, with an incidence of 0.13% in autopsy series.1 These tumors typically involve left-sided valvular structures, and can be associated with serious complications such as myocardial infarction, stroke, and sudden death.2
Diagnostic work-up of cardiac tumors typically includes echocardiography and additional radiographic imaging such as cMRI or CT of the chest. Recent reviews indicate that a correct diagnosis can be obtained with cMRI in 97% of patients, although 42% provide a differential diagnosis.3 Typical clinical presentations can range from asymptomatic patients to those with sequelae from outflow tract obstruction, or systemic or pulmonary emboli.1,2
Definitive management of large cardiac tumors in children involves complete surgical resection.4 Although rhabdomyomas have been known to spontaneously regress without intervention or after partial resection, recent studies advocate for surgical intervention in some patients, depending on tumor size and location, as a prophylactic strategy to prevent mass-related potentially fatal complications such as tumor embolization, severe valve regurgitation or stenosis as the mass impinges on the atrioventricular valve orifice, or ventricular arrhythmias, regardless of the presence of symptoms.1,5 In recently published studies, operative mortality for surgical resection has been reported to be between 4.2-7% in all histotypes, and as low as 2.4% in benign histotypes.1,5,6 These outcomes would support resection in patients when indicated, given the acceptable mortality risk.
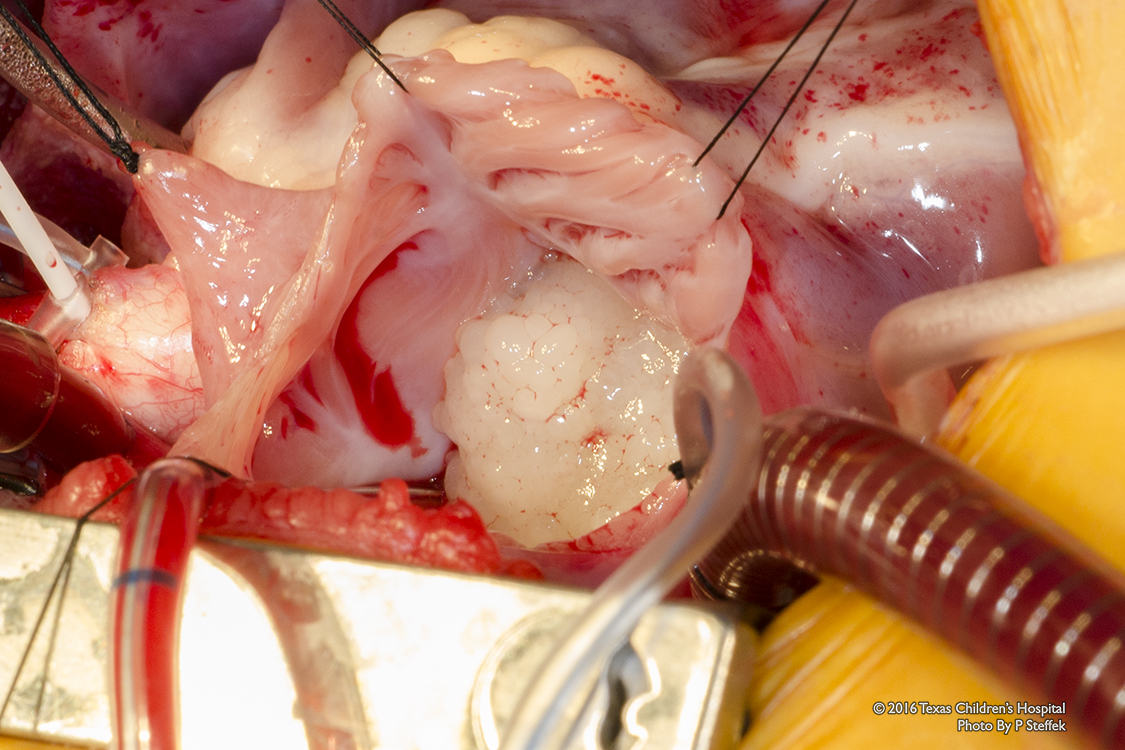
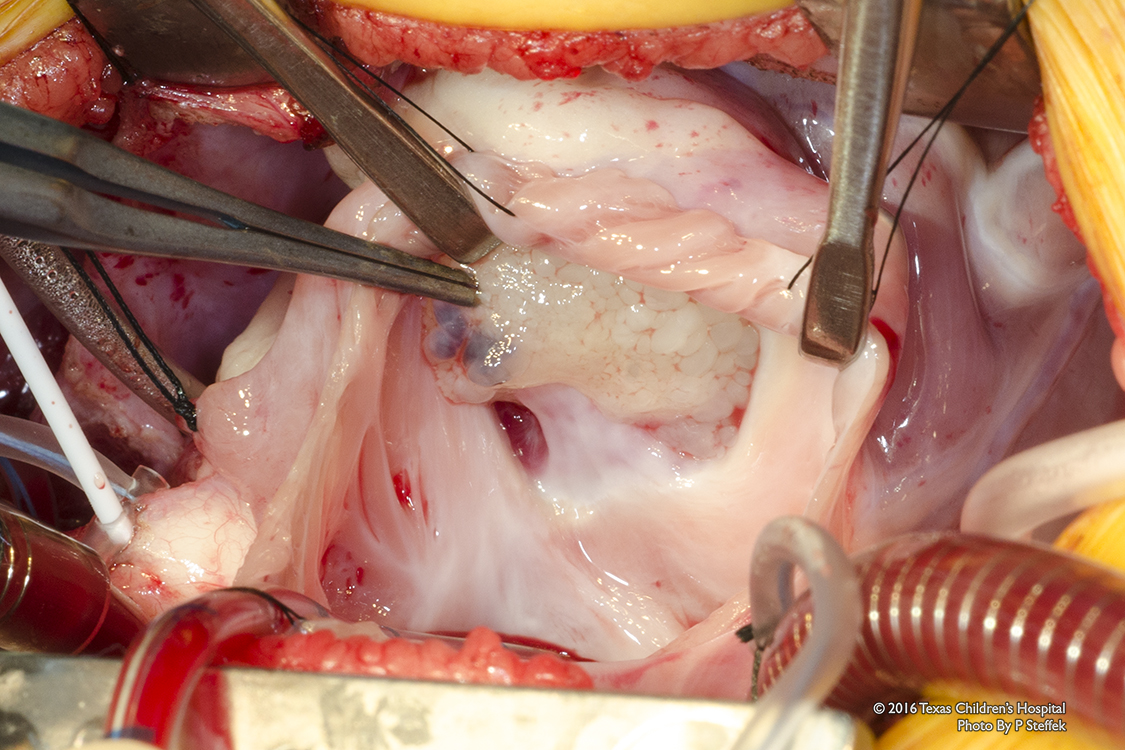
In our particular case, rhabdomyoma was excluded in our differential diagnosis based on cMRI characteristics. Despite the lack of symptoms at presentation, we proceeded with surgical resection due to the unlikelihood of spontaneous regression, with concern for embolic phenomena and potential hemodynamic compromise from RV inflow or outflow obstruction. Pre-operative transesophageal echocardiogram (TEE) indicated that the mass originated from the septal leaflet of the tricuspid valve. On cardiopulmonary bypass, the mass was inspected through a right atriotomy and found attached to the tricuspid valve septal leaflet and its chordae (Figures 1,2,3). Frozen section was consistent with a papillary fibroelastoma, and the remainder of the mass was entirely resected. Subsequent to resection of the mass, the septal leaflet appeared restricted with inadequate leaflet coaptation. A tricuspid annuloplasty was thus performed. Post-operative TEE indicated the presence of mild tricuspid regurgitation with normal biventricular systolic function. The patient did well and was discharged home after an uneventful hospital stay.
Figure 1: Surgical intraoperative initial view of the intracardiac mass looking through the right atrium
Figure 2: Surgical intraoperative view through the right atrium, showing attachment to the septal leaflet of the tricuspid valve
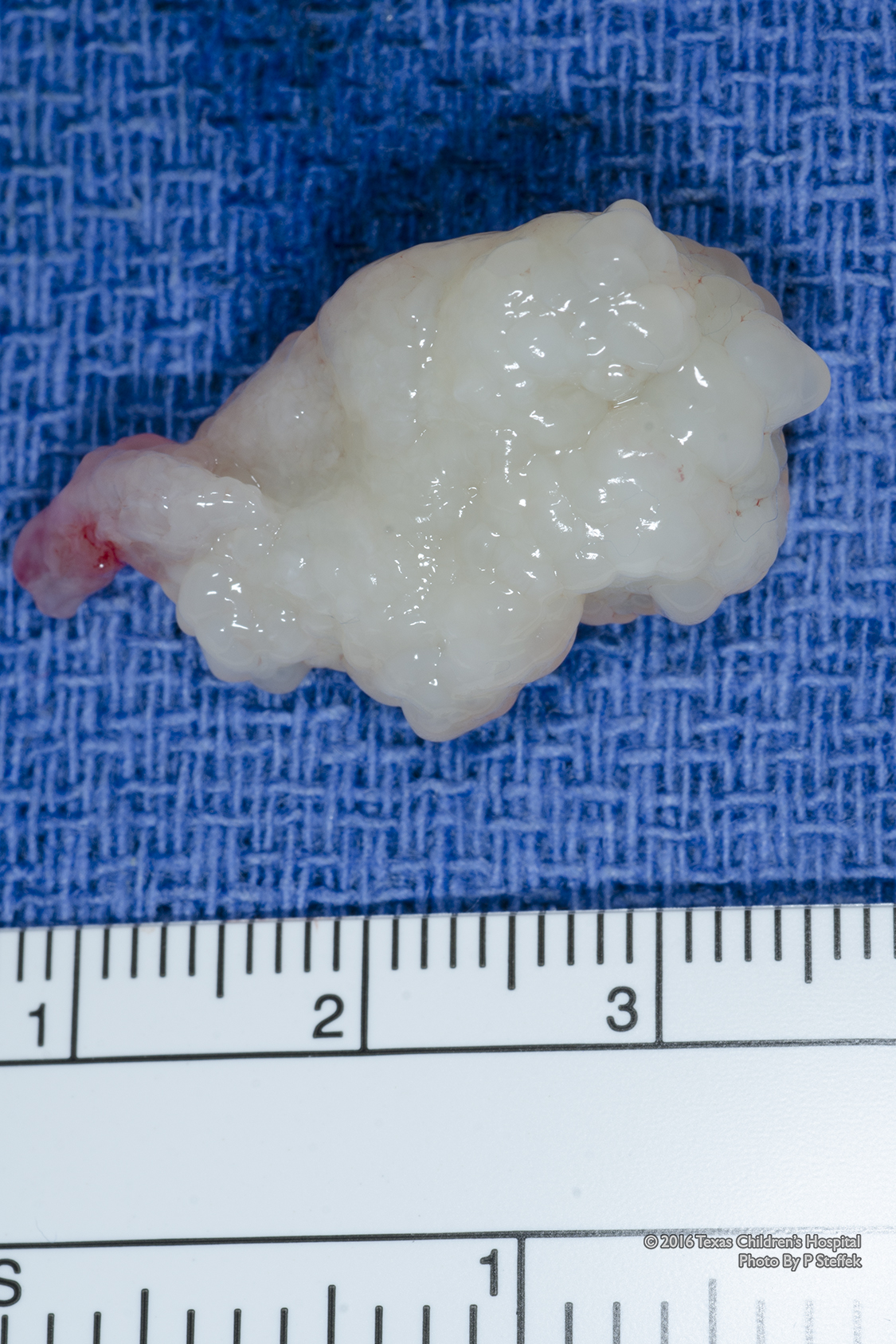
Figure 3: Pathology specimen of the mass, papillary fibroelastoma, approximately 3cm x 2cm
References
Padalino MA, Vida VL, Boccuzzo G, et al. Surgery for primary cardiac tumors in children: early and late results in a multicenter European Congenital Heart Surgeons Association study. Circulation 2012;126:22-30.
Karimi M, Vining M, Pellenberg R, Jajosky R. Papillary fibroelastoma of tricuspid valve in a pediatric patient. Ann THorac Surg 2013;96:1078-80.
Beroukhim RS, Prakash A, Buechel ER, et al. Characterization of cardiac tumors in children by cardiovascular magnetic resonance imaging: a multicenter experience. J Am Coll Cardiol 2011;58:1044-54.
Unusual Cancers of Childhood Treatment (PDQ(R)): Health Professional Version. PDQ Cancer Information Summaries. Bethesda (MD) 2016.
Walter EM JM, Sander F, Hartmann B, Ekkernkamp A, Hetzer R. Primary cardiac tumors in infants and children: surgical strategy and long-term outcome. Ann Thorac Surg 2016. [Epub ahead of print]
Bielefeld KJ, Moller JH. Cardiac tumors in infants and children: study of 120 operated patients. Pediatr Cardiol 2013;34:125-8.