A Patient With a History of HTN and Hyperlipidemia Was Referred For a Dyspnea Evaluation
A 68-year-old woman with a history of hypertension and hyperlipidemia was referred to cardiology for an evaluation of dyspnea. The patient had been taking the following medication:
- Aspirin 81mg daily
- Hydrocholorothiazide 25mg daily
- Lisinopril 40mg daily
- Atenolol 50mg daily
- Rosuvastatin 40mg daily
She had been and continues to be relatively active, but noticed shortness of breath when walking > 5 blocks especially up hills several months ago. Assuming that the patient's dyspnea was her anginal equivalent, her internist decided to order an exercise stress test with nuclear imaging. The patient had no smoking history and her uncle died from the complications of a post-operative CVA while undergoing surgical bypass grafting surgery for severe CAD at age 68. Her resting HR was 72 bpm, and BP 128/70.
- Cr 1.1 mg/dL
- Hgb 13.8 g/dL
- LDL 101 mg/dL
- HDL 47 mg/dL
|
||||||

{kind=link}
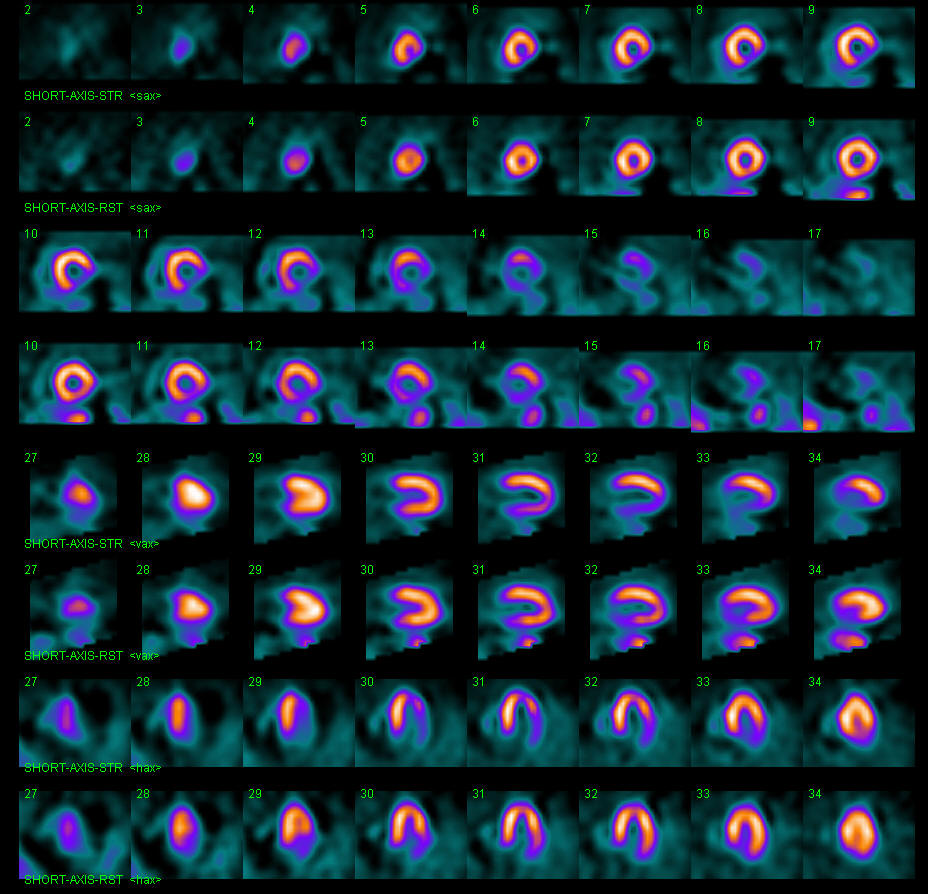
She reached > 85% maximum predicted heart rate and stopped for fatigue and shortness of breath five minutes into the test. Her electrocardiogram revealed 3mm horizontal ST-segment depressions that resolved seven minutes into recovery. The SPECT portion revealed a medium-sized moderate to severe reversible perfusion defect involving the basal and mid inferolateral, apical lateral and basal anterolateral walls (Figure 1). The percent ischemic myocardium was estimated to be 20%.
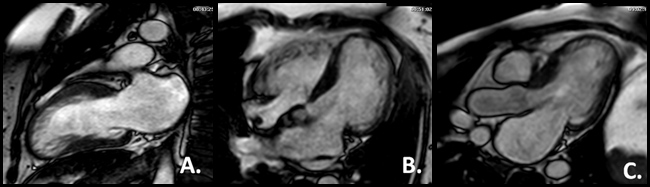
The consulting cardiologist advised coronary angiography which revealed (Figures 2-4):
- mLAD 60%
- Proximal D2 80%
- OM1 80%
- Proximal RCA 80%
- Mid RCA 90%
- Mid RCA 80%
- Distal RCA 30%
What is the best next step in the management of this patient?
Show Answer