A 23-month-old, 10 kg Caucasian male (body surface area [BSA] =0.49), with left ventricle noncompaction (LVNC) cardiomyopathy was found to have an acute decrease in left ventricle assist device (LVAD) filling after having been relatively stable on support for 10 days.
This infant was diagnosed in utero to have prominent left ventricular (LV) trabeculations, congenital complete atrioventricular (AV) block with prolonged QT interval and pulmonary valve stenosis, requiring dual chamber epicardial pacing at 6 days of age and transcatheter balloon pulmonary valvuloplasty at 4 months. He developed progressive LV dilation and severe LV dysfunction consistent with LVNC cardiomyopathy. He was eventually listed for cardiac transplantation.
The patient was admitted to the cardiovascular intensive care unit for poor perfusion and increasing milrinone requirements, necessitating mechanical ventilation and cardiopulmonary resuscitation for pulseless electrical activity. As a bridge to heart transplant, he underwent implantation of a Berlin Heart EXCOR left ventricular assist device (LVAD) (25 ml pump) concomitant with mitral valvuloplasty, prosthetic pulmonary valve replacement, and epicardial pacemaker placement. The EXCOR LVAD was filling and emptying appropriately for ten days (Video 1A/B) until a sudden acute decrease in the filling was noted which resulted in a low cardiac output state. Prior to the change in device filling, anti-coagulation parameters were within therapeutic range, hypertension was well controlled and patient movement was limited by appropriate sedation and paralysis.
A subsequent echocardiogram is shown in Video 2A/B.
Video 1 A&B: Standard transthoracic short axis and apical 4-chamber views
Video 2 A&B: Short axis and apical views depicting thickened interventricular septum
Which of the following is the next best step in the management of this child?
Show Answer
The correct answer is: D. Abandon LVAD circulation and transition to extracorporeal membrane oxygenation.
The atypical, very thickened interventricular septum (IVS) is suggestive of an infiltrative process such as thrombus, infection, abscess, or hematoma. An infection with abscess formation would present more insidiously and would be associated with other clinical findings. Further imaging would unnecessarily delay definitive therapy in this unstable patient with concerning echo findings. C and D are reasonable answers, but alternate LVAD circuit choices are limited in a 10kg child. Thus, D is the best option.
Due to hemodynamic instability, the patient underwent a repeat sternotomy for extracorporeal membrane oxygenation (ECMO), incorporating the previously placed Berlin inflow and outflow cannulae. The Berlin LV inflow cannula was attached to the venous limb of the ECMO circuit along with a newly placed venous cannula in the right atrial appendage, while the Berlin outflow cannula was connected to the arterial limb of the ECMO circuit. Unfortunately, over the next few days, the patient's neurologic status deteriorated and he eventually expired.
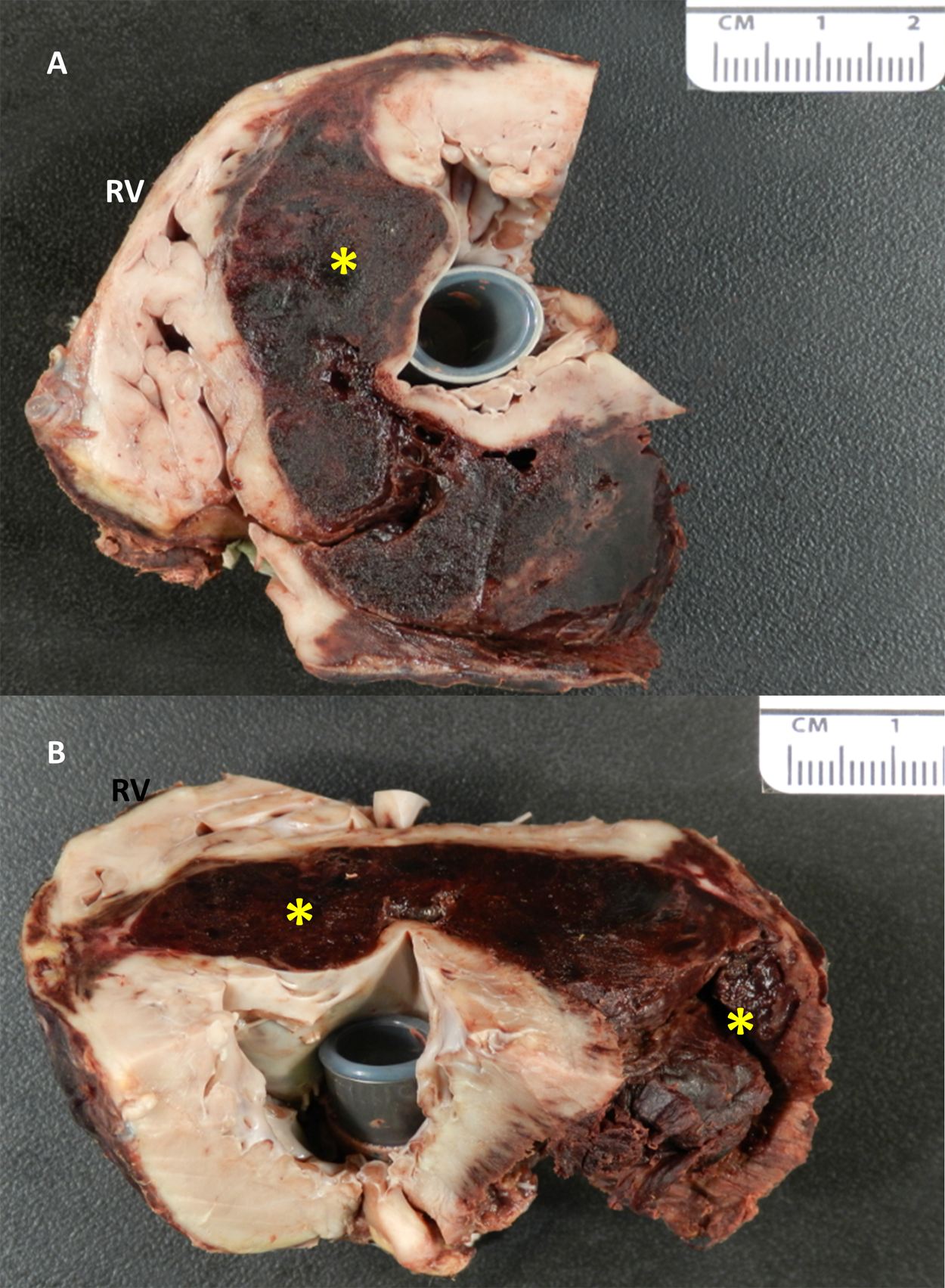
Autopsy confirmed the diagnosis of LVNC cardiomyopathy and endocardial fibroelastosis (EFE). The LVAD inflow cannula was in appropriate position with no evidence of erosion. A massive dissecting hematoma was seen in the interventricular septum, extending into the contiguous subepicardial and posterolateral left ventricle, involving up to 30% of the free wall circumference (Figure 1). There was an acute, transmural myocardial infarction in the left ventricular free wall with subendocardial ischemic necrosis throughout the remainder of all four chambers.
Figure 1 A&B: Postmortem heart demonstrating dissecting hematoma (*) in the septum and
posterolateral left ventricular free wall. The LVAD cannula extends through the LV apex.
This case illustrates a very rare complication of a dissecting intramural hematoma in a pediatric patient on LVAD support.
Pediatric LVAD complications have been well described and include excessive bleeding, thrombus formation, infection, and neurologic injury. Most are readily recognized by clinical or laboratory evaluation. Our case highlights the role of echocardiography in diagnosing serious complications and sudden changes in device performance. A dissecting intramyocardial hematoma is an uncommon device complication that should be included in the differential diagnosis when suboptimal device performance is noted in a child on LVAD support.