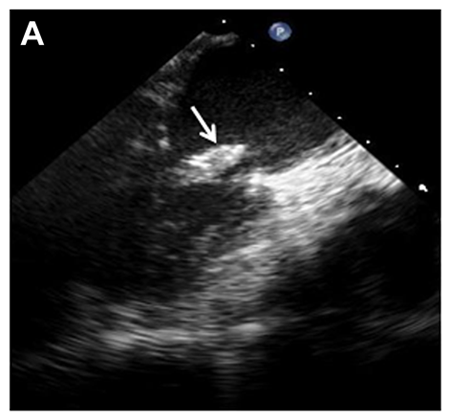
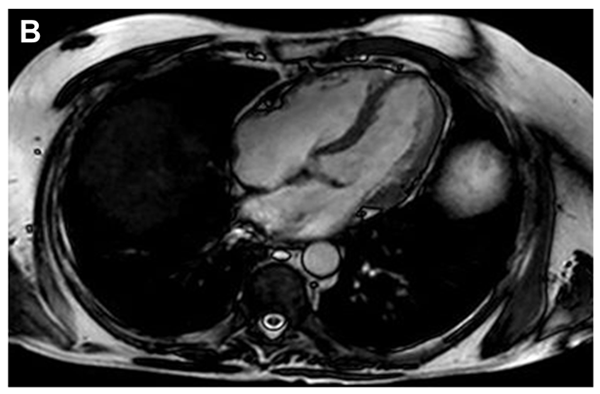
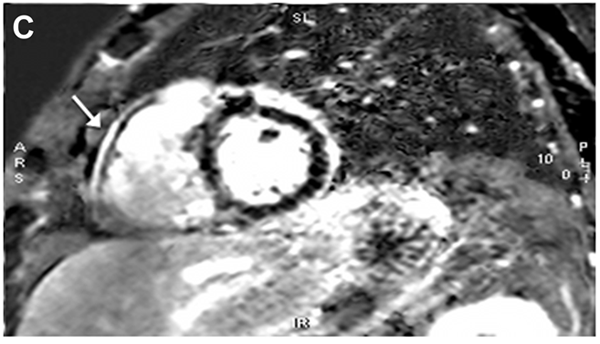
A 57-year-old Caucasian farmer presents with fatigue, weight gain, edema, progressive dyspnea, orthopnea and migratory arthralgias for 18 months. His past medical history included type II diabetes mellitus, hypertension, hyperlipidemia, remote Hodgkin's lymphoma s/p splenectomy and chest radiation, seronegative rheumatoid arthritis on immunosuppressive therapy (prednisone, methotrexate, and previously etanercept), and recent deep venous thrombosis on fondaparinux. Physical exam is notable for fever (temperature 39.1C), jugular venous distension and a positive Kussmaul's sign. Laboratory values were notable for leukocytosis (WBC 17.35), anemia (hgb 9.9) and elevated inflammatory markers (ESR 106, CRP 10.6). TEE showed mitral (Figure A; Video 1) and tricuspid valve vegetations. Cardiac MRI showed evidence of constrictive pericarditis with pericardial thickening and diastolic septal bounce (Figure B; Video 2); delayed pericardial enhancement (Figure C) and septal flattening (Video 3). Serum Whipple's PCR returned positive.
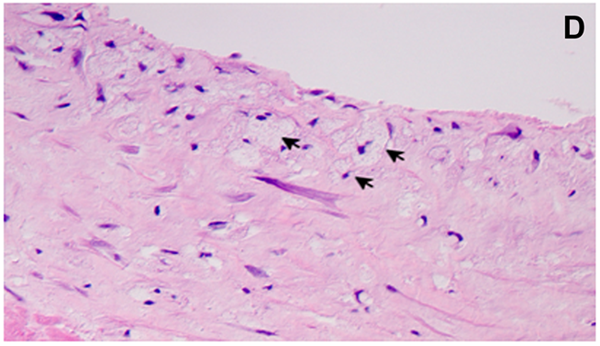
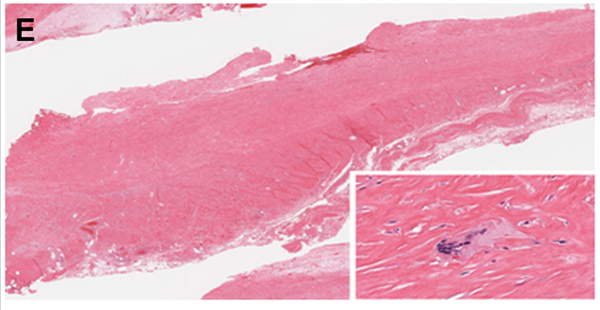
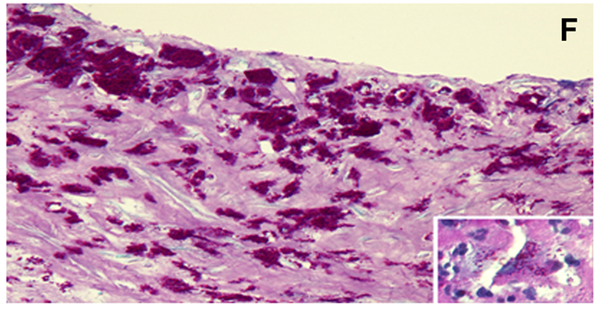
He was initiated on TMP/SMX and IV ceftriaxone and underwent pericardiectomy, MV replacement and TV vegetation removal with subsequent symptomatic improvement. Pathology showed foamy microphages on H&E staining (Figure D) and T.Whipplei-filled macrophages on PAS staining of MV tissue (Figure E), and fibrous pericarditis (Figure F) with PAS-positive organisms. Whipple's disease is an important consideration in patients with exposure risk (such as soil exposure) and the appropriate constellation of symptoms.
Figure A
Figure B
Figure C
Figure D
Figure E
Figure F
Video 1
Video 2
Video 3
Which of the following statements concerning Whipple's disease is false?
Show Answer
The correct answer is: A. All patients with cardiac involvement of Whipple's disease exhibit classic non-cardiac symptoms of Whipple's disease.
Whipple's disease was first described in 1907 by George Hoyt Whipple1. It is a chronic multi-systemic infectious disease caused by Tropheryma whipplei2. T.Whipplei is a Gram-positive, soil living organism. The most common symptoms of classical Whipple's disease (cWD) include weight loss, hypoalbuminemia, diarrhea, arthralgia and anemia2.
Cardiac involvement was first described in 1952 by Upton3. Clinical cardiac involvement is relatively frequent and estimated at 20-55%4 in different case series, with an even higher rate of pathologic involvement estimated at 79% in an early case series3. All layers of the heart (pericardium, epicardium and myocardium) could be involved4, with at least one case of isolated Whipple's pericarditis without endocarditis described5. Patients with infective endocarditits or pericarditis due to T. whipplei may have no symptoms of the cWD6. TWIE (Tropheryma whipplei infective endocarditits) often does not meet the clinical criteria for infective endocarditis using the Duke's Criteria6. The diagnosis is usually established by analysis of explanted heart valves using PCR, culture, and/or immunohistology7. In a study of systemic T. Whipplei in 142 patients at a reference center in Marseille, France published by Lagier in 2010, it was found that 80% of the patients had classic Whipple's disease and 11% (16 patients) had endocarditis7. The epidemiologic and clinical characteristics of those patients with TWIE were as follows: 100% male, mean age of 60.2 years, 31% on immunosuppressive therapy, 69% with arthralgia and 81% with cardiac vegetation7. Evaluation of 1,135 cardiac valves in 2 Germany University centers from 2000-2007 revealed T. whipplei as the 4th most common pathogen for endocarditis (16 cases – accounting for 6.3% of endocarditis cases)6.
The complications resulting from the cardiac involvement in Whipple's disease could be fatal, therefore early diagnosis and treatment are clearly warranted. Antibiotic treatment should include one of the following agents8,9 IV ceftriaxone, meropenem, or penicillin G for 2 weeks; followed by oral sulfamethoxazole/trimethoprim for 12 months OR doxycycline + hydroxychloroquine orally for at least 18 months. Pericardiectomy and/or replacement of the affected valve (if endocarditis is present) are usually indicated4 in addition to systemic antibiotic therapy.
We recommend considering the diagnosis of TWIE especially in males in their sixth or seventh decade of life with a long history of arthralgia, new onset heart failure and echocardiogram showing valvular endocarditis or pericardial disease10.
References
Whipple, G.H. A hitherto undescribed disease characterized anatomically by deposits of fat and fatty acids in the intestinal and mesenteric lymphatic tissues. Bull Johns Hopkins Hosp. 1907; 18: 382–391
Moos V, Schneider T. Changing paradigms in whipple's disease and infection with tropheryma whipplei. Eur J Clin Microbiol Infect Dis. 2011;30(10):1151-1158. PMID: 21461659
McAllister HA, Fenoglio JJ. Cardiac involvement in Whipple's disease. Circulation. 1975;52:152–6
Elkins C, Shuman TA, Pirolo JS. Cardiac Whipple's disease without digestive symptoms. Ann Thorac Surg. 1999;67:250–1
Tariq Iqbal, Alan Karovitch, John Veinot, Raphael Saginur, Luc Beauchesne. Whipple's disease with constrictive pericarditis: A rare disease with a rare presentation. Can J Cardiol. 2009 March; 25(3): e89–e91
Geissdorfer W, Moos V, Moter A, et al. High frequency of tropheryma whipplei in culture-negative endocarditis. J Clin Microbiol. 2012;50(2):216-222. PMID: 22135251
Lagier JC, Lepidi H, Raoult D, Fenollar F. Systemic tropheryma whipplei: Clinical presentation of 142 patients with infections diagnosed or confirmed in a reference center. Medicine (Baltimore). 2010;89(5):337-345. PMID: 20827111
Feurle GE, Junga NS, Marth T. Efficacy of ceftriaxone or meropenem as initial therapies in whipple's disease. Gastroenterology. 2010;138(2):478-86; quiz 11-2.
Schneider T, Moos V, Loddenkemper C, Marth T, Fenollar F, Raoult D. Whipple's disease: New aspects of pathogenesis and treatment. Lancet Infect Dis. 2008;8(3):179-190. PMID: 18291339
Love SM, Morrison L, Appleby C, Modi P. Tropheryma whipplei endocarditis without gastrointestinal involvement. Interact Cardiovasc Thorac Surg. 2012;15(1):161-163. PMID: 22499804