An 18-year-old woman, who is a basketball player on a scholarship at a local university and has no significant past medical history, presents with chest pain and palpitations. Symptoms are described as dull, burning, retrosternal chest pain and tachypalpitations. She denies any syncope or near-syncope. She undergoes an initial evaluation for the chest discomfort, which includes an electrocardiogram (ECG) and an echocardiogram. This reveals a structurally normal heart; however, her ECG reveals the presence of a delta wave consistent with presumed Wolff-Parkinson-White (WPW) syndrome. She undergoes a treadmill myocardial perfusion imaging study that demonstrates normal perfusion and cardiac function on imaging, and there is no inducible tachyarrhythmia on the exercise portion. However, her delta wave remains manifest throughout the exercise period.
She is referred to electrophysiology (EP) for consultation. A 24-hour Holter monitor also reveals the presence of persistent pre-excitation. She is taken to the EP lab where a standard three-catheter EP study reveals pre-excitation with a short his-ventricular (H-V) interval of 25 milliseconds. When on high-dose isoproterenol, supraventricular tachycardia (SVT) cannot be induced; however, a brief episode of atrial fibrillation (AF) is induced without rapid ventricular response. Finally, catheter movement induces a temporary 2:1 atrioventricular (AV) block with persistent pre-excitation on the conducted beats.
Which of the following describes the next most appropriate step in management?
Show Answer
The correct answer is: E. Defer ablation and clear the athlete to return to competitive activity after a 10-14-day recovery period.
The salient observations from this EP study include the following: there is no inducible SVT induced, and when AF was induced, there is no rapid ventricular response. This indicates that the accessory pathway does not place the patient at high risk of sudden death, and does not require ablation.1 The observation that the pre-excitation persists after mechanical induction of transient 2:1 AV block is particularly important. This indicates that not only is the pathway close to the AV node, it originates below the AV node. In fact, this is diagnostic of a rare fasciculoventricular (FV) pathway that does not cause arrhythmias or require ablation.2,3
Answer option A is incorrect because this pathway is essentially part of the normal conduction system. Any attempt at ablation would likely result in complete AV nodal block and require a permanent pacemaker implantation, which would prohibit the patient from participating in competitive athletics.
Answer option B is incorrect because this pathway does not cause arrhythmias and is not demonstrated to conduct AF at a rapid rate.
Answer option C is incorrect because antiarrhythmics are contraindicated without the presence of symptomatic arrhythmias.
Answer option D is incorrect because this pathway does not lead to arrhythmia.
Answer option E is correct. This patient undergoes a trial of a proton pump inhibitor, which completely resolves her chest pain, and she is cleared to return to college athletics. At one-year follow-up, she has had no symptoms or events, and her pre-excitation pattern remains on her ECG.
This case is important as it highlights a potential adverse outcome from failing to recognize these rare variants of pre-excitation that can mimic WPW syndrome and may lead to attempted treatment with ablation or inappropriate exclusion of athletes from competitive athletics.
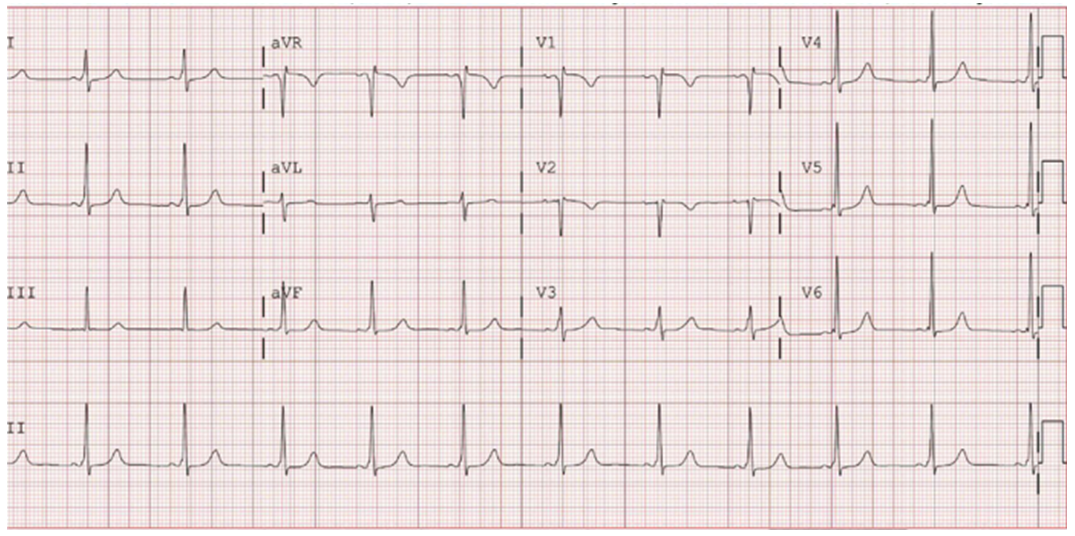
Figure 1: Baseline ECG Demonstrating Pre-Excitation Consistent With WPW Pattern
Based upon surface ECG localization criteria, this accessory pathway is located in the anteroseptal region. A radiofrequency ablation in this region is in close proximity to the AV node, and carries a significant risk of iatrogenic heart block that could necessitate pacemaker placement. This is particularly concerning for this patient as she is not only young, but also a collegiate athlete and would not be able to compete in basketball if this potential complication occurred.
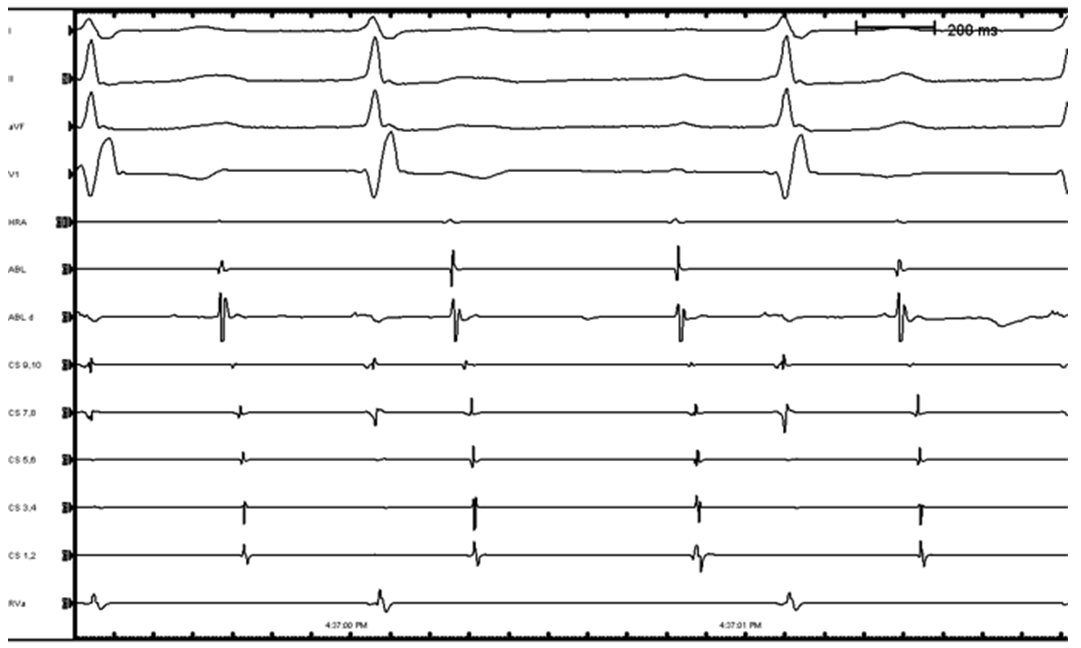
Figure 2: Intracardiac Electrograms From This EP Study
The first four leads are surface ECG. HRA = high right atrium; His = bundle of His recording; CS = coronary sinus recording; RVA = right ventricular apex recording. Electrodes on the catheters are either numbered as pairs (1,2) or as proximal (p), middle (m), or distal (d). This recording demonstrates AF as evidenced by the irregular R-R interval and no consistent electrogram on the HRA catheter. At the end of the tracing, the patient spontaneously converts to normal sinus rhythm, and the final beat demonstrates a clear P wave on the surface ECG. Note that the degree of pre-excitation does not change from beat to beat despite the irregularity of the rhythm. The caliper measurement showed the Shortest Pre-Excited R-R Interval (SPERRI) at 301 msec. Guidelines suggest that a value greater than 250 msec is associated with a low risk of sudden cardiac arrest and ablation is not mandatory (see Figure 4 for diagram).
Figure 3
During catheter manipulation near the AV node, a temporary 2:1 block is induced. Note the presence of pre-excitation on all conducted beats, and the absence of pathway conduction during the time when the AV node is blocked. This single maneuver essentially proves the existence of a pathway that exits below the AV node, in this case a FV pathway. This is an important diagnostic finding, as these FV pathways are benign and are not associated with a risk of sudden death. Since these pathways do not cause any arrhythmia, it is not recommended to attempt to perform radiofrequency ablation, as the risk of AV injury is high and there is no therapeutic benefit to elimination of this pathway.
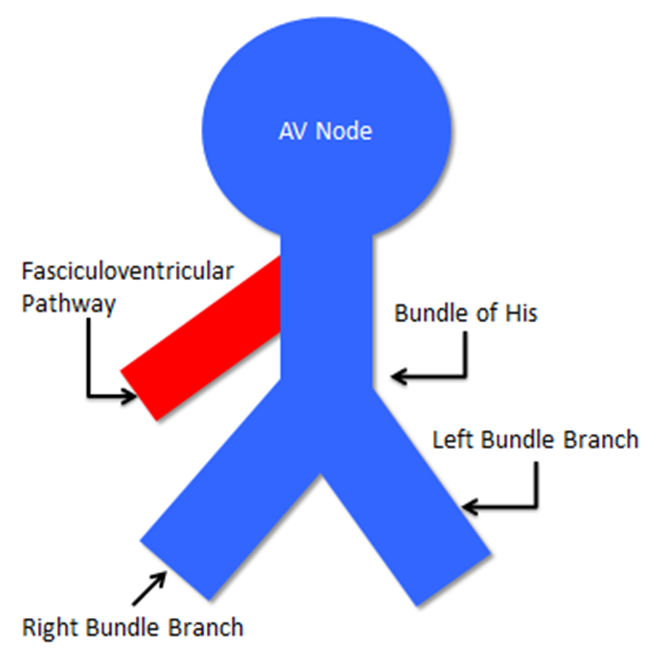
Figure 4
This diagram demonstrates the normal conduction system in blue and the FV pathway in red. These are short pathways that connect the bundle of His directly to the right ventricular myocardium, which produces a very short H-V interval, typically less than 35 msec. As opposed to most other pathways in WPW syndrome that connect the atrial to the ventricle, this pathway only connects the bundle of His to the ventricle; therefore, the ventricle is protected from excessively rapid conduction of atrial arrhythmias, as these arrhythmias can only conduct down the AV node.The views expressed in this article are those of the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government.
As coauthor, I am a military service member. This work was prepared as part of my official duties. Title 17 U.S.C. 105 provides that "Copyright protection under this title is not available for any work of the United States Government." Title 17 U.S.C. 101 defines a United States Government work as a work prepared by a military service member or employee of the United States Government as part of that person's official duties.
References
Cohen MI, Triedman JK, Cannon BC, et al. PACES/HRS expert consensus statement on the management of the asymptomatic young patient with a Wolff-Parkinson-White (WPW, ventricular preexcitation) electrocardiographic pattern: developed in partnership between the Pediatric and Congenital Electrophysiology Society (PACES) and the Heart Rhythm Society (HRS). Heart Rhythm 2012;9:1006-24.
Park DS, Giovannone S, Cecchin F, Chinitz LA. Preexcitation on surface ECG: Where is the accessory pathway? Heart Rhythm 2014;11:2124-5.
Suzuki T, Nakamura Y, Yoshida S, Yoshida Y, Shintaku H. Differentiating fasciculoventricular pathway from Wolff-Parkinson-White syndrome by electrocardiography. Heart Rhythm 2014;11:686-90.