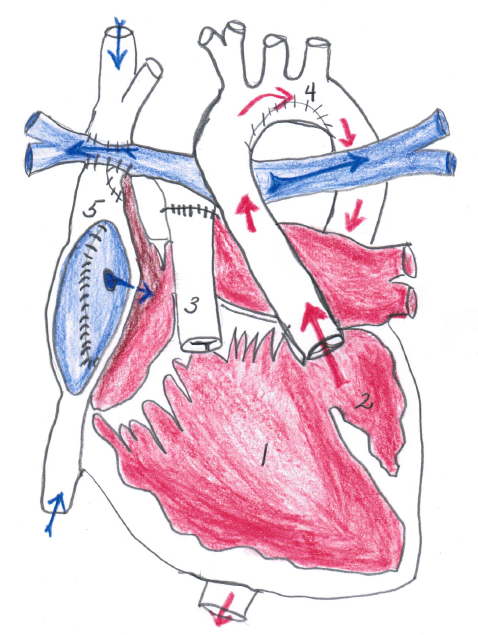
A 12-year-old active male presents for his routine annual cardiology follow-up with the following diagnoses: L-looped double inlet left ventricle (LV) with "corrected" transposition and coarctation, status/post (s/p) resection of the LV outflow tract and end-to-end repair of a coarctation, and s/p a fenestrated Fontan procedure done nine years ago. The result of this patient's anatomy and surgical palliation is that the LV pumps as the systemic ventricle, and, in the absence of a pumping right ventricle, a cavo-pulmonary anastamosis allows passive flow to the lungs. Often in these sorts of palliations, a fenestration is left as a pressure "pop off" from the passive Fontan connection into the systemic circulation, which can result in mild patient desaturation, particularly during times of exertion (Figure 1).
Figure 1
The patient and his family have just returned from a hiking trip, where they increased their elevation by ~500 feet (peak altitude >10,000 feet) and walked a total of 5 miles. His father states that his son walks this distance frequently without looking cyanotic or short of breath. He would like to continue as an Eagle Scout, which requires this type of activity.
On physical exam, he appears well, albeit slightly cyanotic. His oxygen saturations are 85%, and he is slightly clubbed. The blood pressure is normal, the resting heart rate is 60 bpm and junctional. The cardiac exam is remarkable for a normal S1 and a single S2. There are no murmurs. Of note, his hematocrit is 50% and stable.
The echocardiogram shows a well-functioning single ventricle with no regurgitation of the atrioventricular (AV) valves. The Fontan baffle is well-visualized, and there is a fenestration shunting from right to left with a peak gradient of 16 mm Hg. The branch pulmonary arteries are well-visualized with phasic flow.
Which of the following additional pieces of information would you like to have prior to "clearing" this patient for high altitude hiking and camping?
Show Answer
The correct answer is: G. B, C and D.
Cardiac catheterization with possible intervention, Holter monitor, and Exercise stress test.
This patient is mildly cyanotic and polycythemic, the etiology of which differs from that of an Eisenmenger's physiology, where there is involved pulmonary vasculopathy which prevents adequate perfusion. As previously mentioned, this patient's cyanosis is due to a direct right (venous blood) to left (arterial blood) shunt, which induces the bone marrow response of polycythemia. His resting oxygen saturations are lower than anticipated from a Fontan fenestration, although he is living at high altitude. Additionally, the gradient across the Fontan fenestration is somewhat high. He should be evaluated for any obstruction in the Fontan circuit, the formation of venovenous collaterals, and should undergo "test occlusion" of the fenestration.
The Holter monitor is a non-invasive method to evaluate the cardiac rhythm and rate variability during his day-to-day activities. Patients with L-looping are at high risk for heart block. Additionally, he is at risk of sinus node dysfunction due to the Fontan procedure.
An exercise stress test allows evaluation of his chronotropic and metabolic response to exercise, yielding data to support exercise recommendations. While an EP study may be done, in the setting of a Fontan baffle, it may prove difficult, and the risk may not outweigh the benefit.
Simply restricting an adolescent with complex congenital heart disease (CHD) from physical activities may have several lasting effects. The psychological benefits and sense of accomplishment gleaned from safe activity are documented. There are also data to support the fact that adults with CHD who exercise with regularity are more likely to be gainfully employed. Additionally, regular exercise in any group of individuals is likely to provide weight control benefits and improved quality of life.
Currently there are no data to support exercise limitation in patients with single ventricle Fontan palliations. The Fontan is a passive conduit and therefore, patients with Fontan physiology are at risk for the development of thromboembolism. Exercise is one logical solution to avoid venous stasis of a sedentary lifestyle. In fact, restriction is this population is deleterious and contributes to the published experience of exercise impairment in this group by enhancing deconditioning, as exercise restriction somehow becomes medically advisable.
In addition, this patient underwent coarctation repair, leaving him at risk of systemic hypertension and the long-term complications of vasculopathy. Avoidance of this specific complication is another argument for life-long exercise.
Once the patient's anatomy is confirmed, (that is, no Fontan baffle obstruction, possible occlusion of the Fontan fenestration, query for venovenous collateral, assessment of ventricular function, atrioventricular valvar regurgitation, and residual coarctation), his EP and his exercise capacity have been evaluated and found to be satisfactory, this patient should be allowed to exercise to his own self-limitations. At the age of 12-years, he should be given information regarding his anatomy, advice on exercise and long-term outlook as he transitions at the age of 18-years to an adult congenital heart specialist. He should be reminded to be extremely conscientious with his hydration. Hydration is imperative at higher altitudes, and is also crucial to patients with polycythemia in order to avoid the known complications of a higher hematocrit.
References
Sutherland N , Jones B, d'Udekem Y. Should We Recommend Exercise after the Fontan Procedure? Heart Lung Circ 2015;24:753-68.
Hsu, DT. The Fontan operation: the long-term outlook. Curr Opin Pediatr 2015;27:569-75.
Müller J, Ewert P, Hager A. Increased aortic blood pressure augmentation in patients with congenital heart defects - A cross-sectional study in 1125 patients and 322 controls. Int J Cardiol 2015;184:225-9.