Thank you for visiting ACC.org. Please note that this item was published more than 5 years ago and therefore its content may be outdated. For more current information on this topic, we encourage you to visit our Congenital Heart Disease and Pediatric Cardiology Collection page.
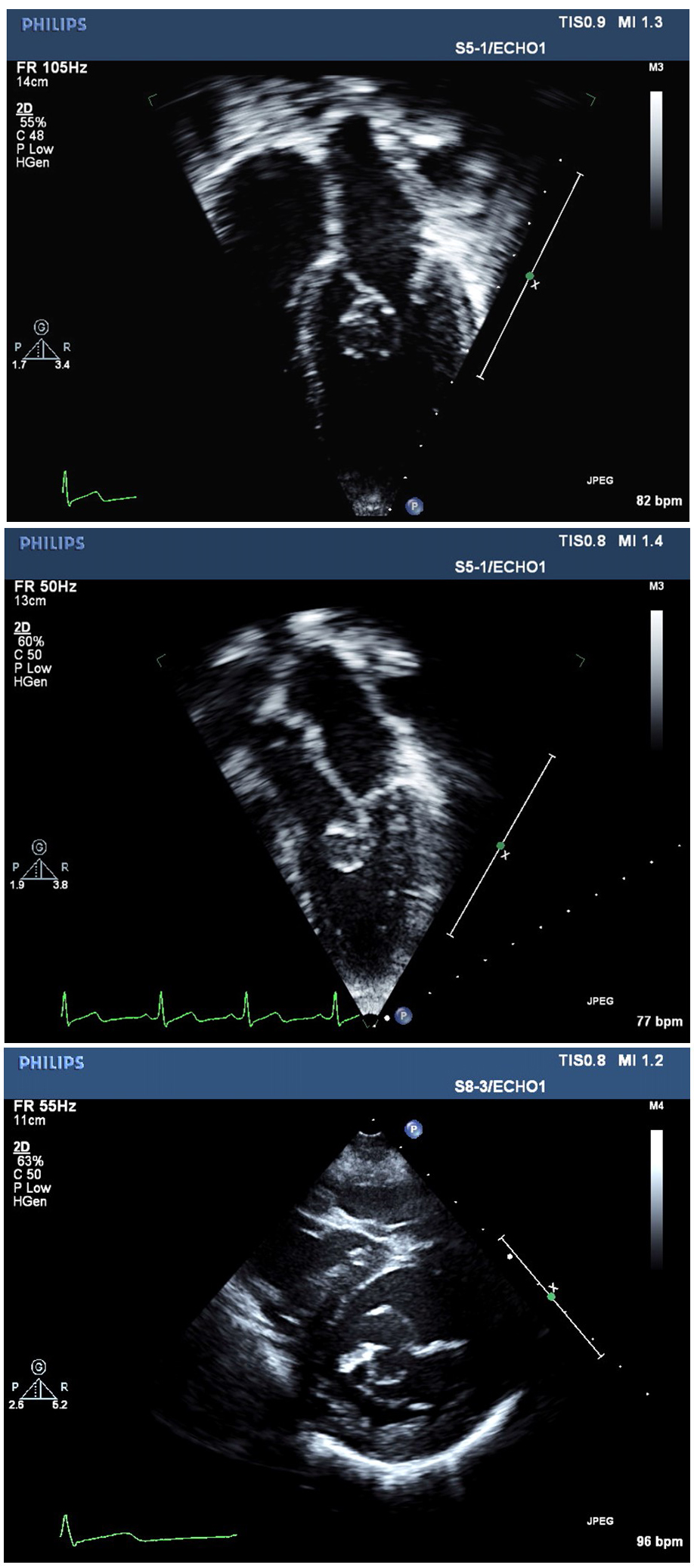
An 8-year-old boy was referred to the cardiology clinic for left ventricular hypertrophy on a routine electrocardiogram, performed as part of the work-up for attention deficit hyperactivity disorder. His parents report declining exercise tolerance and shortness of breath in the preceding year, a change from his previous asymptomatic baseline, but deny any other symptoms; vital signs were within normal limits and cardiac exam was unremarkable. An echocardiogram was performed, select clips of which are shown below.
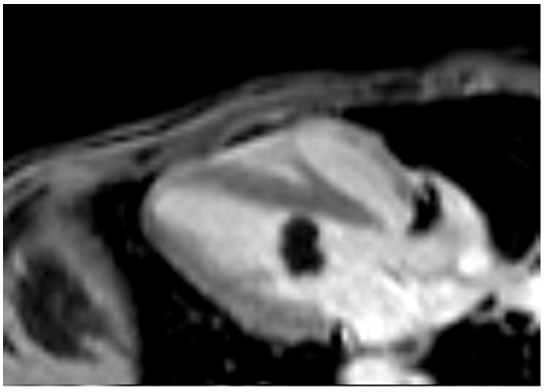
Figure 1: Short Axis View
Which of the following represents the next best step for evaluation of the patient?
Show Answer
The correct answer is: C. Cardiac magnetic resonance imaging with tissue characterization sequences.
The patient has a blood cyst. Small blood cysts (≤2 mm) are a common finding in fetuses and infants. They are found most often on the atrioventricular valves, detected in over 50% of autopsies, with cause of death unrelated to the cyst. These small blood cysts are considered benign and asymptomatic, and are rarely detected after infancy.1 Large blood cysts, as in our patient, are extremely rare in children and adults. Case reports describe such blood cysts occurring on all cardiac valves and attached to all cardiac chambers. Depending on size and location, blood cysts can cause outflow tract obstruction and impaired valve function, and have been implicated in thromboembolic events. Blood cysts have also been detected as incidental findings on echocardiogram.2-7
Primary cardiac tumors are also uncommon in the pediatric population (reported incidence of 0.027% to 0.08%) and the overwhelming majority are benign.8,9 Rhabdomyomas are the most common intracardiac mass in the pediatric population, as compared to myxomas in the adult population.
Cardiac MRI with tissue characterization has enhanced the anatomical assessment of intracardiac tumors, without exposing the patient to ionizing radiation as would be the case with chest and cardiac computed tomography.10-12
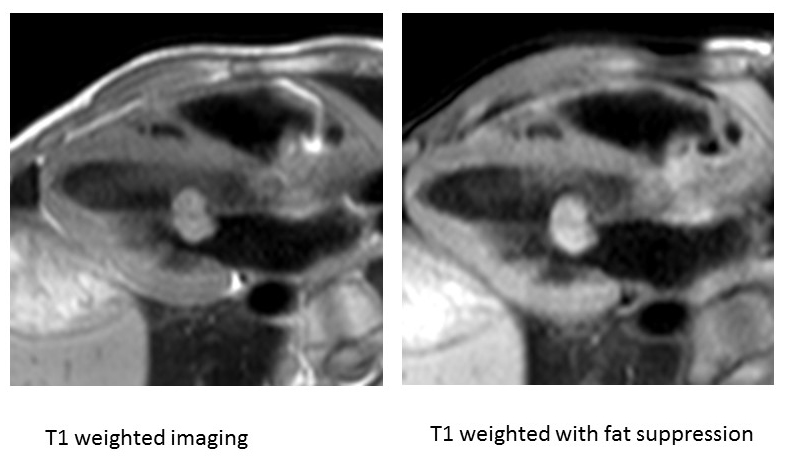
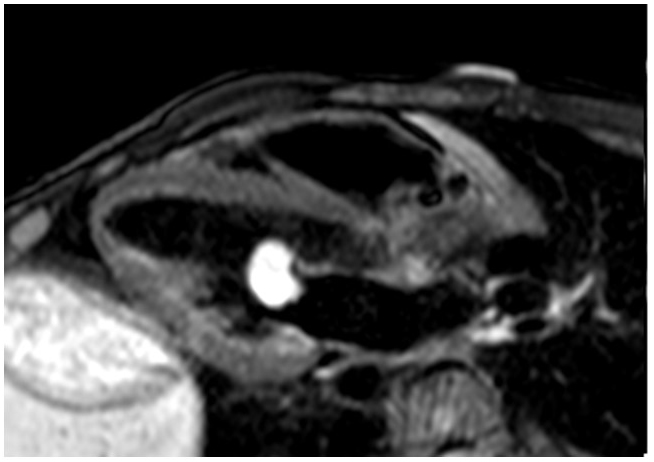
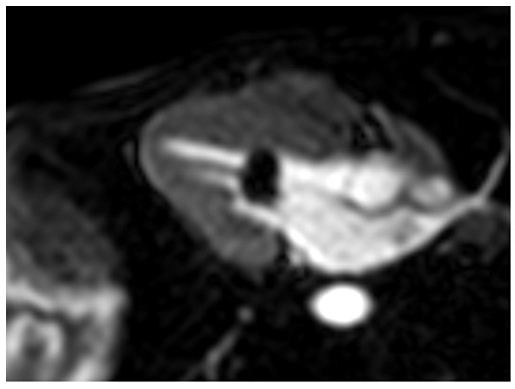
Highlighting the usefulness of a multimodality approach, cardiac MRI with tissue characterization sequences had findings consistent with a blood cyst. Specifically, with T1-weighted imaging the mass was isointense (compared to the normal myocardium) and did not suppress with fat saturation (Figure 2). With T2 weighted imaging and fat saturation, the mass became hyperintense compared to the normal myocardium (Figure 3). Finally, with both first pass perfusion imaging and delayed enhancement the mass was hypointense (Figure 4 and 5).
Figure 2-5: MRI Images of the Blood Cyst
Transesophageal echocardiogram was not necessary given that transthoracic echocardiogram already clearly demonstrated the mitral valve cyst, and in a pediatric patient would require intubation and anesthesia.
High resolution chest and cardiac CT would have shown the mitral valve cyst but would not have allowed for the tissue characterization sequences and would have exposed the patient to radiation.
Stress echocardiogram would not have aided in delineation of the mitral valve mass characteristics.
Cardiac catheterization with biopsy of the mass would be invasive and a biopsy of the mass would result in rupture.
There are no established guidelines for the optimal management of incidental blood cysts. Our patient underwent surgical resection due to the decreased exercise tolerance and possibility of embolization of the mass which has been reported in the literature without incident and the diagnosis of a blood cyst was confirmed on visual inspection during surgical excision as well as by pathology. The patient is currently doing well and is now asymptomatic with exercise.
Video 1
References
Zimmerman KG, Paplanus SH, Dong S, Nagle RB. Congenital blood cysts of the heart valves. Hum Pathol 1983;14:699-703.
Bonenfant F, Essadigi B, Gahide G, Jeanmart H, Farand P. Mitral valve blood cyst detected by multimodality imaging. Can J Cardiol 2014;30:1109.e5-6.
Combaret N, Azarnoush K, Marcaggi X, et al. A blood cyst on the anterior mitral valve leaflet complicated by cerebrovascular stroke. J Heart Valve Dis 2012;21:688.
Dencker M, Jexmark T, Hansen F, Tyden P, Roijer A, Luhrs C. Bileaflet blood cysts on the mitral valve in an adult. J Am Soc Echocardiogr 2009;22:1085.e5-8.
Minato H, Manabe T, Masaki H, Kawahara Y. Blood cyst of the pulmonary valve in an adult: report of a case and review of the literature. Human Pathol 1997;28:252-5.
Park MH, Jung SY, Youn HJ, Jin JY, Lee JH, Jung HO. Blood cyst of subvalvular apparatus of the mitral valve in an adult. J Cardiovasc Ultrasound 2012;20:146-9.
Hauser AM, Rathod K, McGill J, Rosenberg BF, Gordon S, Timmis GC. Blood cyst of the papillary muscle: clinical, echocardiographic and anatomic observations. Am J Cardiol 1983;51:612-3.
Isaacs H. Fetal and neonatal cardiac tumors. Pediatr Cardiol 2004;25:252-73.
Nadas AS, Ellison RC. Cardiac tumors in infancy. Am J Cardiol 1968;21:363-6.
Prakash A, Powell AJ, Geva T. Multimodality noninvasive imaging for assessment of congenital heart disease. Circ Cardiovasc Imaging 2010;3;112-25.
Beroukhim RS, Prakash A, Beuchel ER, et al. Characterization of cardiac tumors in children by cardiovascular magnetic resonance imaging: a multicenter experience. J Am Coll Cardiol 2011;58:1044-54.
Kiaffas MG, Powell AJ, Geva T. Magnetic resonance imaging evaluation of cardiac tumor characteristics in infants and children. Am J Cardiol 2002;89:1229-33.